
Thiamine (vitamin B1) is an essential micronutrient responsible for key reactions involved in the conversion of the foods we consume into the chemical energy substrate requisite for cellular function, adenosine triphosphate (ATP). Absent sufficient ATP, all sorts of metabolic functions become disordered leading to the disease processes that dominate western medicine. Chronic inflammation, altered immune function, hormone dysregulation, cognitive and mood disorders, and dysautonomias, all can be traced back to insufficient thiamine > inefficient mitochondrial function, reduced ATP, and the compensatory reactions that ensue.
Among the most common but least well-recognized contributors to thiamine deficiency is the regular consumption of a high carbohydrate/highly processed food diet. Although most of these foods are enriched or fortified with thiamine, perhaps staving off more severe deficiencies, the density of sugars overwhelms mitochondrial capacity to process these foods, both the thiamine and any other potential nutrients are excreted, while the carbohydrates themselves are stored as fat for future use. High-calorie malnutrition is a common contributor to thiamine deficiency in obesity but also may develop in presumed healthy athletes whose diets focus heavily on high carbohydrate intake.
Thiamine, along with other B vitamins is often deficient in vegetarian and vegan diets as well. Not only do fruits, vegetables, and carbohydrates contain minimal, if any, thiamine, but some have anti-thiamine factors and are high in what are called oxalates. Anti-thiamine factors found in some fruits and vegetables interfere with the absorption or digestion of thiamine. Oxalates are mineralized crystals of sorts that tend to build up and store in places like the kidneys (kidney stones), but also may store and cause problems anywhere in the body like bones, arteries, eyes, heart, and nerves. Effective oxalate metabolism and clearance requires thiamine. Since vegetarian and vegan diets are also carbohydrate intensive, thiamine deficiency and oxalate issues may be compounded. Thus, a number of common diets not only contain reduced thiamine content but cause an increased need for thiamine by at least three mechanisms; higher carbohydrate consumption overwhelming capacity, which is then magnified by poor carbohydrate and oxalate processing.
Add daily coffee, tea, and/or alcohol consumption to any diet, and whatever thiamine that is consumed is either inactivated by enzymes before being used or is unabsorbable. Add a medication or four and thiamine availability will tank simultaneously with an increased need. Medications both block nutrient uptake and/or increase the need for nutrients by inducing mitochondrial damage. Given that 70% percent of the US population takes at least one medication regularly, while 20% take four or more, it is safe to say, that a good percentage of the population is consuming insufficient thiamine to maintain mitochondrial function and health.
Are We Really Thiamine Deficient?
As an essential nutrient, thiamine must be consumed regularly to maintain sufficient concentrations. The question is how much thiamine is sufficient to maintain health? Current RDA values for daily thiamine intake suggest a little over a milligram per day is adequate for most adults. If this is true, then the minimum value can be attained through just about any diet including those dominant in highly processed, carbohydrate-dense foods, which are commonly either enriched or fortified with thiamine. Everything from bread to cereals and even junk food like Oreos have thiamine. Per the RDA values, none of us ought to be thiamine deficient and none of us ought to require thiamine supplementation, and yet, many of us are and do. Indeed, several studies, across disparate populations show that even by this minimum standard, deficiency is a serious health problem. From our book:
- 76% of diabetics (type 1 and type 2)
- 29% of obese patients, 49% of post-bariatric surgery
- 40% of community-dwelling elderly, 48% of elderly patients in acute care
- 55% of cancer patients
- 20% ER patients (random sample, UK)
- 33% of congestive heart failure patients
- 38% of pregnant women, more with hyperemesis
- 30% of psychiatric patients
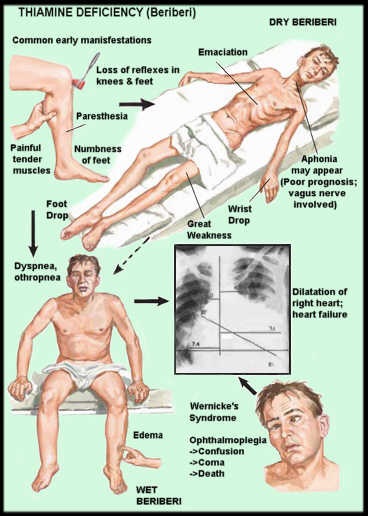
It takes approximately 18 days to completely abolish endogenous thiamine stores in a diet that is completely devoid of thiamine. Except under total starvation, medical or industrial food production mishaps, and experimentally contrived situations, thiamine consumption is never completely abolished. It waxes and wanes by dietary choices and life stressors. According to rodent studies, it takes a reduction of greater than 80% of thiamine stores before the more severe neurological symptoms are recognizable. In humans, these symptoms include those associated with Wernicke’s encephalopathy, the various forms of beriberi, and dysautonomic function. These include but are not limited to: ataxia, changes in mental status, optic neuritis, ocular nerve abnormalities, diminished visual acuity, high-output cardiac failure with or without edema, high pulse pressure, polyneuropathy (sensorimotor), enteritis, esophagitis, gastroparesis, nausea and vomiting, constipation, hyper- or hypo-stomach acidity, sympathetic/parasympathetic imbalance, postural orthostatic tachycardia syndrome (POTS), cerebral salt wasting syndrome, vasomotor dysfunction, respiratory distress, reduced vital capacity, and/or low arterial O2, high venous O2.
With a less severe thiamine deficiency, symptoms are rarely recognized as such and often attributed to psychological manifestations. A not entirely ethical study done in 1942 involving 11 women on a low thiamine diet over a period of ~3-6.5 months found striking symptoms.
- During this time all subjects showed definite changes in personality.
- They became irritable, depressed, quarrelsome, and uncooperative.
- Two threatened suicide. All became inefficient in their work, forgetful, and lost manual dexterity.
- Their hands and feet frequently felt numb.
- Headaches, backaches, sleeplessness, and sensitivity to noises were noted.
- The subjects fatigued easily and were not able to vigorous exertion.
- Constipation was the rule, but no impairment, of gastrointestinal motility, could be demonstrated fluoroscopically.
- Anorexia, nausea, vomiting, and epigastric distress were frequently observed.
- Low blood pressure and vasomotor instability were present in all patients.
- At rest, pulse rates were low (55 to 60 per minute) but tachycardia followed moderate exertion. Sinus arrhythmia was marked.
- Macrocytic, hypochromic anemia of moderate severity (3.0 to 3.5 million red cells) developed in 5 cases.
- A decrease in serum protein concentration occurred in 8 subjects.
- Basal metabolic rates were lowered by 10 to 33 points.
- Fasting blood sugar was often abnormally high.
The study above demonstrated a rapid and dramatic onset of symptoms relative to a diet with limited thiamine. Depending upon caloric intake, the amount of thiamine allowed was approximately 1/3 to 1/5 of the amount recommended by the RDA. Admittedly, the RDA for thiamine is low, to begin with, but even so, this was not a complete absence of thiamine. Since the study took place in the early 1940s, it is difficult to ascertain the specifics of the diet. Nevertheless, it demonstrates a clear association between general health and one’s ability to function, and thiamine insufficiency.
High Carbohydrate Diets Equal Lower Thiamine
More recently, a short and very small study (12 days and 12 participants) of active young men and women (ages 25-30) investigated the relationship between carbohydrate intake and thiamine status. Thiamine was measured in blood, plasma, urine (creatinine), and feces at four time points: at baseline, before the study began, during an adaptation phase where carbohydrate intake represented 55% of the total caloric intake, and during the two subsequent intervention phases, where carbohydrate intake was increased to 65% and 75% of the total caloric intake, respectively. Both caloric and thiamine intake was held constant throughout the study despite the increased intake of carbohydrates. Activity levels were also held constant. Across this short-term study, as carbohydrate intake increased, plasma, and urinary thiamine decreased. Excretion through feces remained unchanged. Transketolase enzyme activity was also measured but remained unchanged. Given the short-term nature of this study, the fact that transketolase remained unchanged is unexpected. In addition to the decreasing thiamine values, there were several changes in lipid profile as well. Despite the short duration of this study, however, the results show a clear relationship between carbohydrate intake and thiamine status; one that would likely be magnified over time and certainly if other life stressors and medical and environmental toxicants were added to the mix.
It is important to note current dietary guidelines suggest carbohydrate consumption should fall between 45-65% of total calories, percentages which, per this study would decrease thiamine availability significantly. From the baseline diet to the 55% adaptation phase, thiamine dropped precipitously, only to drop even further at the 65% phase. A recent study surveying macronutrient consumption showed that average carbohydrate consumption across the US population represented approximately 50% of total caloric intake. Importantly though, the study found that 42% of the carbohydrate consumption came in the form of what researchers termed ‘low-quality carbs’ e.g. sugary processed foods with no nutritional value. Thiamine is only found in pork, beef, wheat germ and whole grains, organ meats, eggs, fish, legumes, and nuts. It is not present in fats/oils, polished rice, or simple sugars, nor are dairy products or many fruits and vegetables a good source. Indeed as mentioned previously, some fruits and vegetables may contain anti-thiamine factors. A diet that is 42% empty calories, that contains limited to no nutritive value, save except what has been added post hoc via enrichment, begs for mitochondrial damage and the illnesses that ensue. And yet, that is precisely the nutritional landscape in which most of us exist.
Admittedly, both studies were very small, but the research connecting thiamine deficiency to ill-health and carbohydrate consumption to thiamine loss is clear. Given the dominance of ultra-processed carbohydrate-dense foods in the modern diet, is likely that high-calorie malnutrition underlies much of the chronic illness that plagues western medicine. To learn more about thiamine deficiency and the havoc it wreaks on health: Thiamine Deficiency Disease, Dysautonomia, and High Calorie Malnutrition.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, and like it, please help support it. Contribute now.




You might be interested in































{kind=link}