Maple Syrup Urine Disease at 52 Years of Age

There are some rare diseases that appear at birth known as inborn errors of metabolism. Their symptoms are nonspecific in most cases and each of them is unrecognizable clinically, with some exceptions. All of them are genetically determined. Most of them can be spotted from a tiny sample of blood that is sent to a central laboratory in each state in the United States and is known as “a screening test”. Perhaps the best known in the general population is one called phenylketonuria, also known as PKU. This disease is estimated to occur once in 10,000 births. If the infant is placed on a special diet he or she can grow up to be normal. If the diet is not initiated, as close to birth as possible, the infant will become intellectually disabled. This obviously emphasizes the importance of the screening test. Another of these rare diseases is known as Maple Syrup Urine Disease. It gets its name because the urine smells exactly the same as the characteristic odor of maple syrup. Although the abnormal genes responsible for the disease are known, the cause of the odor is not. It is just as deadly as PKU, but is estimated to occur only once in 100,000 births. The diet restrictions are extremely complex, involving protein metabolism.
An Infant with Maple Syrup Urine Disease
Fifty-two years ago, when I was a pediatrician at Cleveland Clinic, a physician from southern Ohio called and spoke to the secretary of the Department of Pediatrics. He said that he had an infant boy that he would like to refer because he smelled most peculiar. The secretary made a provisional diagnosis of Maple Syrup Urine Disease (MSUD) and assigned the case to me. It became a departmental joke because she was absolutely correct. There was no available commercial diet for a rare disease of this nature. It had to be constructed from scratch. The mechanism for the disease had only been described relatively recently. Because the genes control some important aspects of protein metabolism, the abnormality makes it necessary to devise a severely restricted protein diet. If such a patient has too much protein, the metabolic abnormality causes severe brain dysfunction, usually resulting in seizures and death. Well, such a diet was constructed and I was able to preside over his health for several years. As the family hailed from West Virginia, I inevitably lost sight of him. With the best of care, accurate treatment for such a complex problem is impossible. If the infant survives, it can be expected that there will be some degree of intellectual disability.
Half a Century Later
To my extreme surprise, I recently received an email from a physician in Virginia. He had been able to locate me through another physician who was known to each of us. He informed me that my former patient was now 52 years old and he had this extraordinary story to tell.
The physician, who had special knowledge of this kind of disease, said that he had been called to see the patient (JD) who was 30 years of age at that time and in a state of coma. The mother of JD was in possession of the details of the original diagnosis and his history. Evidently he had not remained on the restrictive diet, a fact that itself was unusual. However, his mother had given him “lots of fruit juice” if ever he had, as she described it, “acted drunk”. This, of course, had removed the dietary protein until stability returned. He had had no unusual crises until a strep throat had affected his abnormal metabolism and precipitated coma. JD was moved to a hospital where the proper treatment was established under the care of the consulting physician who had continued to follow his course. He told me that JD is able to carry on a reasonable conversation, fits in well with his community, mows the church grass and is a firm fan of NASCAR. He developed gout in his 40s and has since developed type II diabetes.
Lessons to be Learned
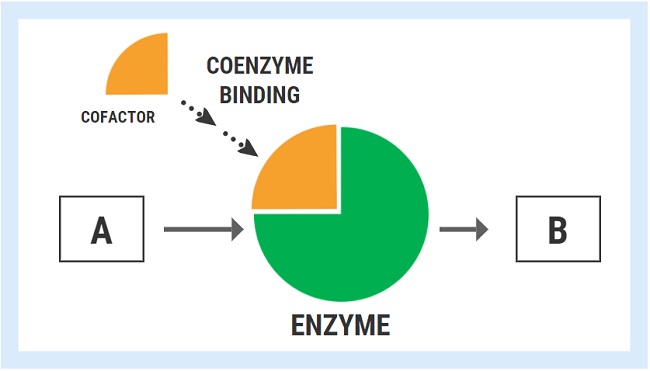
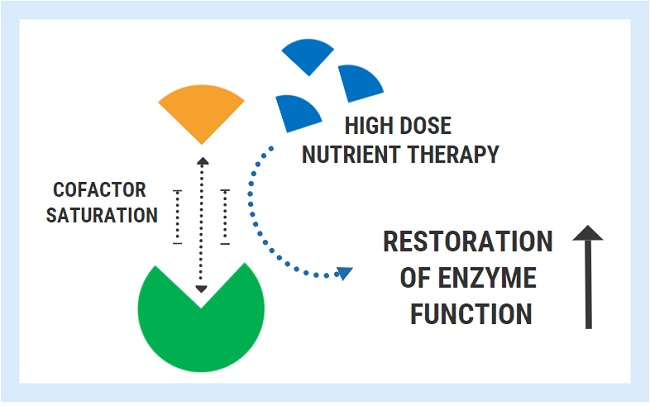
This genetically determined disease is caused by failure of an enzyme that has an integral part to play in protein metabolism. As has been mentioned a number of times in posts on this website, many enzymes require a vitamin and/or a mineral, known as a cofactor to the enzyme. The defective enzyme that causes MSUD requires thiamine and magnesium as cofactors. But, as has also been mentioned in other posts, both are vitally important in sugar metabolism. Gout has long been known to be related to an excess of sugar. The disease was common in Port drinking military officers in the British Indian Army before India became independent. Port wine has a high sugar content in addition to the alcohol. We also know now that thiamine in large doses is vitally important in the treatment of both diabetes and brain disease caused by alcohol. It is logical to conclude that JD really requires therapeutic doses of thiamine and magnesium as epigenetic stimulants to the defective enzyme, at least on clinical trial. This conclusion is reached because other enzymes that require thiamine and magnesium appear to be affected, besides the one responsible for MSUD.
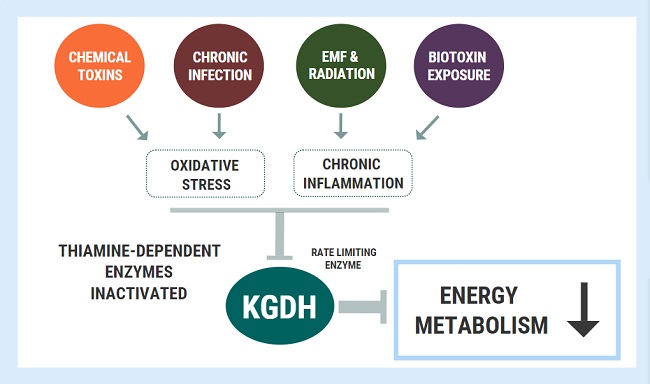
Stressors Evoke Metabolic Crises
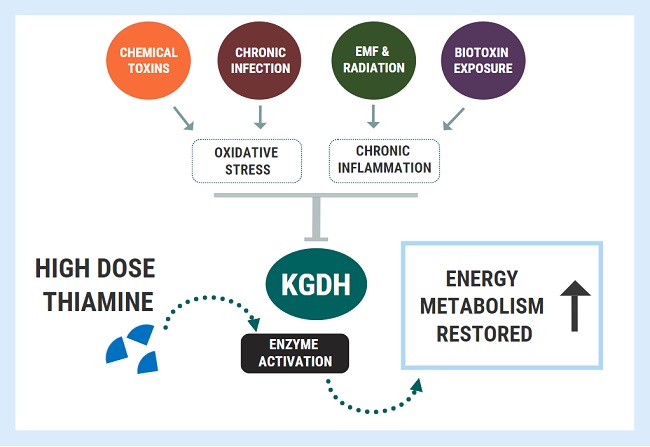
Those who have followed some of the posts in this website will be aware that an infection can act as a stressor. So it was no surprise that JD succumbed to a metabolic crisis as a result of contracting a strep throat. In previous posts we have tried to point out that an infection constitutes an attack on the organism and can therefore be thought of as a source of stress if the exact meaning of that word is applied. It was no surprise to me to hear that he had contracted gout and diabetes in addition to MSUD. Also the truly amazing thing to me is that no thought has been given to why a person with a rare, genetically determined disease has also been affected by two other diseases without thinking that they probably have a cause that is common to all three. He is being treated with a drug for gout and another drug for diabetes. Both gout and diabetes are related to sugar metabolism that is highly dependent on thiamine. The defective enzyme responsible for MSUD requires thiamine.
The point that I am trying to make is that it is the underlying biochemistry that is rapidly becoming vitally important in diagnosis. Yes, it is true that MSUD is a rare and exotic disease, but understanding its underlying principles enables us to think whether these principles are implicated in common diseases. To believe that two or three separate diseases can occur at the same time in one individual is reduction to absurdity, without thinking that they have a common relationship. I passed this idea to the physician who had contacted me and it is his decision whether he tries it or not. The outstanding reason for doing it is that it is impossible to do harm, even with megadoses of thiamine. It would also be a cheap experiment and the only two outcomes would be either some success or no change in the patient’s mental capacity.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
Image by Beverly Buckley from Pixabay.
This article was first published on August 10, 2016.
Rest in peace Derrick Lonsdale, May 2024.




You might be interested in