Pregnancy Toes – What Sugar Does to Feet

Pregnancy toes are really swollen feet and swollen toes. The name stuck in my mind because one of my daughter-in-laws is pregnant and I was sent a photo from her winter vacation in her flip flops in the snow and winter coat—she was not able to put her boots on because of her swollen feet (swollen even in the cold!).
I did not think much about it until she came to visit me yesterday and I noticed the flip flops and her chubby toes. She had “pregnancy toes” again she said. It then suddenly all became clear. I asked her: did you by any chance have any sugar today? And she said “as a matter of fact, yes!”
I reached for my salt pills that I use for my migraines as do all members in my migraine group on Facebook and handed her one. I really should have photographed what happened but I did not think the effect was going to be so fast and so big. Less than 15 minutes after she took the salt pill and a glass of water, her toes went back to normal. We ended up laughing it away. Had she known this, she could have worn her boots in the snow after all!
So what did her pregnancy toes have to do with sugar and salt you may ask? Previously, I quoted from the Harrison’s Manual of Medicine an important paragraph that I repeat here:
…serum Na+ falls by 1.4 mM for every 100-mg/dL increase in glucose, due to glucose-induced H2O efflux from cells. (page 4)
The above means glucose (part of sugar) and sodium (part of salt) are in inverse relationship. As you increase sugar, salt drops and water is sucked out of your cells by sugar like a giant Slurpee machine. The water then collects on the outside of your cells rather than the inside, thereby dehydrating your cells and at the same time make your body swell. Edema is often associated with too much salt, but in fact, it is too much sugar. Being always thirsty is associated with Type 2 Diabetes but it is also associated with not having enough salt in the body since without salt the cells cannot get hydrated.
In light of this fragile balance between sodium and glucose in the blood, are we treating pregnancy edema, gestational diabetes, and other maternity complications, the way we should? Consider that with pre-eclampsia (gestational hypertension), women are told not to eat salt. You can see what happens when we reduce sodium: glucose increases and we also induce an ionic imbalance. This ionic level imbalance is visible (like the swollen toes) and may lead to further complications. There are two problems that we are facing here: first if she does not eat salt, her sodium-potassium pumps cannot work–this may cause migraines and headaches as I often see in my migraine group. Secondly, as you saw the fragile balance between the see-saw action of glucose and sodium, if she stops eating sodium her glucose may increase, causing swelling. This is an interesting theory to ponder – one that merits research.
Sodium and Glucose Work Together
Salt breaks up in the body into sodium and chloride. Sodium attracts water and holds onto it inside the cells. It keeps chloride outside of the cells to ensure proper voltage and electrolyte balance with the aid of potassium. When you eat sugar, the glucose part of it removes the water from the cells via osmotic channels that are too narrow for the sodium ions to exit. Thus, one ends up with a ton of water outside the cells with sodium inside hugging a tiny amount of water. Swelling occurs as the water leaves the cells but remains between cells.
Given the inverse nature of glucose and sodium in the blood, if one is swollen as a result of too much sugar, eating salt will take the water back from sugar and move it back into the cells–as it did for my daughter-in-law’s pregnancy toes. What is important in this information is this:
- If you feel swollen after eating sweets, you need to eat salt and drink a bit of water to reduce your swelling.
- If you have Type 2 Diabetes or are hypoglycemic, eating a salty meal can give you a major sugar crash and land you in the hospital!
- Eating sugar of any quantity will dehydrate your cells and you and make you run to the toilet every 30 minutes.
Because glucose takes water out of the cells, the edema that follows increases extra-cellular water and causes swelling in the body. This extra-cellular water needs to be reabsorbed into the circulation for the kidneys to be eliminated. To be reabsorbed, sodium is necessary since without sodium, the cells cannot operate their voltage gated sodium pumps and so the gates cannot open to grab glucose to take it into the cells and to get the water back into the cells. I think you can already see the contradictions in the logic of reduced salt: the mom-to-be is told to not eat salt, this causes extra-cellular water and swelling, which needs salt to be reabsorbed into her cells for clearance by the kidneys but which she is not allowed to eat. This way ionic level balance is not possible and chain reactions may occur with negative consequences. She may have protein leaching into her urine, extra hard kidney work, and a whole other long chain of complex events may kick in to make pregnancy a rather unpleasant experience risking the health of the fetus.
The amount of extra-cellular water is very hard for the body to get back into circulation without salt and may take days, taxing the kidneys with the volume of water leaving and increasing pressure on the blood vessels from the outside, causing high BP. However, as the volume of water is leaving the body finally, this reduces blood pressure. When a pregnant woman’s blood pressure drops as a result of all that water leaving, the dehydrated blood cells carry less oxygen. This indicates reduced oxygen for both her and the baby.
By telling mothers to reduce salt intake, glucose increases, which increases blood pressure (BP) rather than reduces it. The similar phenomenon happens in gestational diabetes. In gestational diabetes (and gestational hypoglycemia as well) the sugar level is unstable and is either too high or too low, respectively. Should the mother-to-be eat a salty pickle (as cravings always dictate pickles), she may end up in a major sugar crash and in the hospital for immediate treatment.
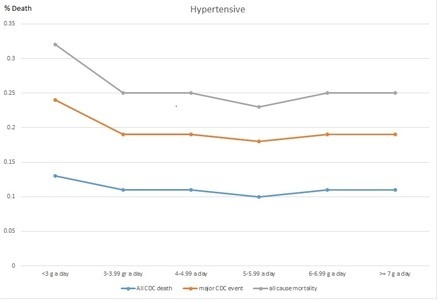
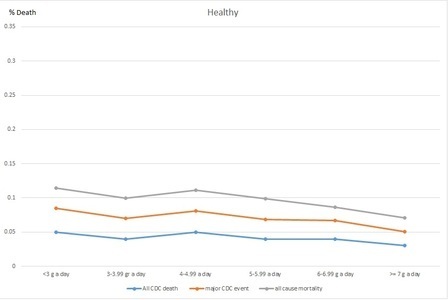
The balance between sodium and glucose is very fragile and extremely quick changing as you could see on my daughter-in-law’s foot. Interestingly we now also know that salt does not increase blood pressure but sugar does and so a reduced salt diet automatically increases blood pressure because of the glucose and sodium inverse connection and sugar’s dehydrating properties. Reduced salt also increases triglycerides (Graudal, 2011), causing a lot of problems for people with preexisting heart conditions. So by reducing the salt intake of the mothers to be, are we creating diabetic mothers and/or babies? Babies have been born with diabetes 2!
Is it possible that we are giving the wrong advise to pregnant women about salt and sugar? It’s an interesting question to pose and further research is badly needed. Knowing that salt and sugar are in inverse proportion in the blood, one may suggest eating them together. In fact, eating them together is a much better idea than eating sugar alone. It is best to not eat sugar at all but if you must eat sugar, consider eating salt too.
Sources:
Effects of low sodium diet versus high sodium diet on blood pressure, renin, aldosterone, catecholamines, cholesterol, and triglyceride. Graudal et al., Cochrane Database Syst Rev. 2011 Nov 9; (11).
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.




You might be interested in