

One of the more pervasive, and frankly, annoying myths about menopausal women is that they cannot build muscle after a certain age. The argument goes that as certain hormones decline, so too does the ability to build muscle. On the surface, that seems like a reasonable argument. Indeed, there have been an endless number of studies that suggest hormone decline, in both males and females, negatively influences muscle mass and strength. Ditto for the opposite – increasing certain hormones increases muscle development for both males and females. Why else would we have entire industries devoted to the development of hormones for use in competitive sports and sub-industries whose sole purpose is to find ways to circumvent the detection of those products? Yes, all else being equal, certain hormones impact muscle development more positively in higher concentrations and more negatively in lower concentrations. Does that mean however that hormones are the sole contributors to muscle development, or as the menopausal research always seems to conclude, that the state of diminishing hormone concentrations as we age and move through menopause is enough to hamper or prevent muscle development in women? No. Absolutely not.
Like so many aspects of women’s health research, the connection between declining hormones and declining muscle is spurious at best. It relies on equal parts latent (and not so latent) biases towards women and surrogate markers that may or may not equate directly with muscle and strength. The bias holds that women, in general, have difficulty building muscle compared to men based upon their unique hormonal makeup e.g. lower androgens and higher estrogens, a difference that is magnified with aging. This bias leads to research questions that essentially presume the answer in the framing of the question. That is, the research asks ‘why women have difficulty building muscle’ across menopause or compared to men and not ‘do women have difficulty building muscle.’ The research assumes that women have this issue, and thus, proceeds show us why. It then uses surrogate markers of this supposed muscle-building difficulty, neither defining clearly what constitutes muscle development nor measuring actual muscle development in women who train to build muscle. When the associations between these surrogate markers and the hormone in question is found, usually estradiol, are found, as they so often are, causation is inferred and PR campaigns begin.
This bugs me to no end for a number of reasons, not the least of which, is because it is an asinine way to conduct research, but mostly, because it is logically fallacious. We have made the assumption that women have difficulty building muscle and proceed to demonstrate why. Of course, we are going to find some reasons. We can do that with any research design that assumes the answer in the question. It would be no different than assuming all men are idiots and designing research to find out why. It is offensive and it is wrong, and yet, this is the standard course of most research. What is that saying – assumptions make asses out of you and me? Well, research like this makes asses out of us all.

So where is all of this going? Well, yet another study illustrating why menopausal women have difficulty building muscle crossed my desk, replete with the expected PR piece showing grey-haired women lifting the cute and oh-so-cheerfully colored 1lb dumbbells.
To say that I had a negative reaction to it would be putting it mildly. I am not sure why this particular study set me off more than any other though. I mean these types of studies and their associated PR are dime a dozen in this field and this one was not any worse than any of the others that I have read. In fact, it had some cool technology that allowed them to assess scientifically sexy surrogate markers, the muscle stem cells called satellite cells. They ‘discovered’ that muscle stem cells in women do indeed respond to hormones, as they do in men, and as all cells do. And they do indeed diminish and die off absent those hormones, both in cell culture and in ovariectomized rodents, making recovery from injury difficult. They also found that in four of the five older women tested, none of whom was reported to engage in muscle-building activities, muscle stem cells numbers naturally declined across time, as did estradiol concentrations. There was no information on the fifth woman. Groundbreaking right? This explains why women have difficulty building muscle as they age, right? Sure, if you don’t know anything about how hormones work or how muscle gets built.
Hormone Basics
To understand why this and studies like it that attribute the actions of a single hormone like estradiol to a more global function like muscle development fall short, we have to understand a thing or two about how hormones work in real life versus how we measure them in the lab. I would argue that much, if not all, single-hormone-to-single-variable research fails, no matter the hormone or the variable because the actions of a single hormone are fundamentally incongruent with how hormones behave in real life. Hormones never, ever, ever act in isolation. Each hormone’s existence is entirely dependent upon its sister hormones up and down the metabolic chain, and thus, they are all in a constant and interdependent state of communication and activity. Not only that, hormones interact with the totality of one’s internal chemistry, responding to and signaling information about things like nutrient availability/unavailability, immune and inflammatory changes, and most importantly, mitochondrial energetics. So no, a single hormone study will never come close to approximating the complexity of interactions in real life. And it doesn’t take an advanced degree to understand this. A quick Google image search hormone synthesis shows us quite clearly how much more complicated hormone to variable interactions are. Here is one of many illustrations.
Figure 1. Steroid hormone synthesis in the adrenal cortex.
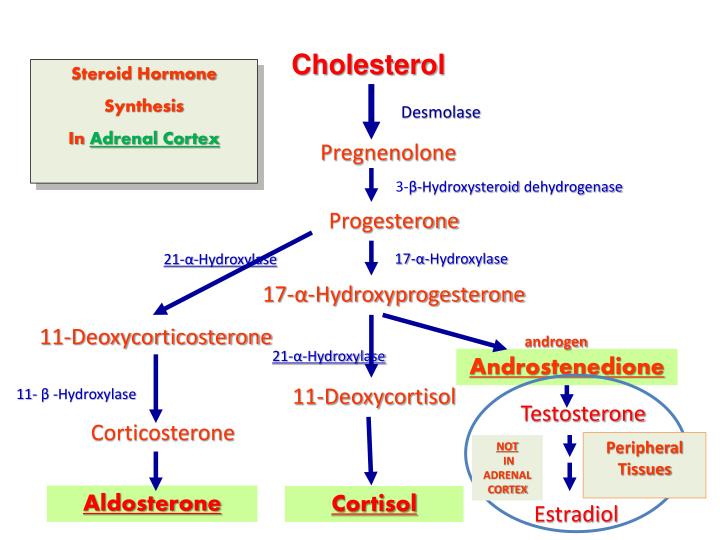
This is an oversimplified version of what is really happening. Take a look at this image to appreciate the complexity of steroid hormone synthesis. Even so, from the image to the left, we can see that all steroid hormones are synthesized from cholesterol (yes, that cholesterol, the one we are all so happy to block with drugs) to pregnenolone (in the mitochondria), and then to progesterone and on through a complicated network of enzymes to the more commonly recognized steroid hormones like testosterone and estradiol.
These figures should tell us a few things about hormones. First, hormone metabolism is damned complicated. While understanding the mechanisms of action of a single hormone is an important endeavor, we must always remember that hormones never act in isolation and so any results we may attribute to that single hormone, are necessarily limited and often flawed. Second and following from the first point, all steroid hormones are connected to each other in some way or another. That means, the concentration of one hormone invariably affects and is affected by, everything else around it, both its downstream metabolites and through feedback control mechanisms, its upstream precursors.
Third, neither progesterone nor estradiol are exclusively female hormones. Progesterone is a precursor hormone for everything else and so, yes, men have it too, and estradiol derives directly from testosterone, and so both men and women have both testosterone and estradiol. What determines how much of each and what directions these metabolic pathways take is determined by enzyme activity, which is determined first by genetics and then by where, what tissue or gland, the enzyme is located within the body. In the ovaries, we get more pregnane (progesterone) and estrane hormones (the estrogens collectively), and in male gonads, the paths shift towards the androgens, but in neither are those the ‘only’ hormones produced by those glands. Moreover, in both males and females, the adrenal glands produce a full complement of androgens, some estrogens, and what are called glucocorticoids (cortisol) and mineralocorticoids (aldosterone). Fat cells synthesize, store, and react to estrogens, in males and females. While muscle cells synthesize and respond to a full complement of hormones, not just androgens, and do so, in what is called a sexually dimorphic manner. Interestingly, after a single bout of exercise testosterone is upregulated in both male and female muscle, while estradiol production is increased in males only. So how is it that estradiol is solely responsible for muscle in women?
I should also note that the brain synthesizes and responds to steroid hormones. Not only does the brain have the entire collection of enzymes to synthesize its own hormones from scratch, but because steroid hormones are lipid-soluble, those produced in the body easily cross the blood-brain barrier (and for the more nerdy among us, even the less fat-soluble sulfated hormones cross via transporters). Then, of course, are all of the environmental estrogens that we are exposed to on a daily basis, but that is another topic for another day. Needless to say, hormones can be synthesized, and thus act, anywhere.
Finally, steroid hormones do things, this perhaps, is the most important point. They can turn things on or off directly or they can fuss with the volume of a signal, turning it up or down. How they do this involves binding to receptors. Some of these receptors are on the cell membranes (fast-acting, volume control) and others are inside the cell nucleus (slower acting, gene regulation). Steroid hormones are promiscuous in their choice of receptors. While they have preferences for and tend to bind more tightly to their own receptors (estradiol to estrogen receptors, for example), they may also bind to other receptors (progesterone to mineralocorticoid receptors or deoxycorticosterone [substrate for cortisol] to androgen receptors, for example). See here for a brief description. Bottom line, we all have the same hormones, just different concentrations relative to genetic sex, enzyme activity, and gland presence/absence.
I point all of this out because laboratory studies tend to focus their work on the actions of a single hormone using a variety of common methodologies. They expose cells to hormone and hormone-free media measuring the differences between the two or they remove the hormone-producing gland, knock out a gene or two involved in its synthesis or the synthesis of its receptors, and again measure effects without the hormone and then added back. While experimentally valid approaches, in vivo, that is in real life, hormones do not act in isolation, and barring some very specific genetic issues or medical treatments, single hormones are never reduced to zero. So when we see studies that claim to show that X hormone is responsible for Y behavior using these methods, we have to remember that while it may be implicated in said behavior, the real relationship is far more complicated than experimental design allows.
It’s Never Just One Hormone
With all of this in mind, let us consider the role of estradiol in health. Estradiol, like many hormones, is a necessary component of human physiology. We have estrogen receptors all over the body and the brain. Both men and women produce estradiol and have estrogen receptors, though men to a much lesser degree. Cells exposed to estradiol are going to do something, usually turn something on, but also, especially when concentrations get too high, turn something off. An interesting side note, the estrogen receptor is considered to be the first hormone receptor to evolve, dating back some 450 million years ago. The progesterone receptor evolved next. Both receptors appear to have evolved well after their respective hormones. How exactly that worked, I am not sure. Importantly though, estradiol does stuff. So studies that tell us cells do something in response to estradiol and die off in its complete absence are interesting, but not necessarily indicative of anything else but what is happening in that particular experimental environment.
Similarly, the common ovariectomy and estradiol add-back protocols used in research with female rodents, though unfortunately closer to reality, as hundreds of thousands of women are castrated annually, still fall short but for different reasons. Castrating an animal or a human woman causes a violent, immediate decline in hormones (not just estradiol, but all of the hormones produced by the ovaries), and as we would expect it to, that violent decline in hormone availability causes problems -everywhere. Resources have to be reallocated for survival. In the immediate aftermath of castration, cell death is to be expected. Again, and of course, the add-back therapy will diminish some of the symptoms and prolong the life of the cells in question. Remember though, estradiol receptors are everywhere and are required for cell function (and mitochondrial function). Period. If we remove it, cells die. If we add back, they don’t die as quickly. We could do the same thing with other steroid hormones and get the same result to varying degrees because those receptors exist too and therefore impact cellular function as well. It is never just one hormone. Keep repeating that. It is never just one hormone.
Does any of this suggest that estradiol is THE HORMONE involved in female muscle development? No. It suggests what we expect it to suggest, that estradiol is involved in muscle development, just like a whole bunch of other variables are also involved but rarely measured in combination. Other hormones, diet, and the single most overlooked variable it seems, actual strength training, play role in muscle development. As such, we would expect any one of these variables, alone or in combination to positively affect any number of the surrogate markers tested within these protocols.
Will You Get to the Muscle Part, Already?!
Now that we know estradiol does stuff but not in isolation, can we really attribute the menopausal decline in estradiol to this seemingly entrenched idea that women of a certain age have difficulty building muscle? No, we cannot for the reasons stated above, but also, because we have yet to define either what building muscle constitutes or what ‘difficulty’ means. Does it mean that with the appropriate weight training, menopausal cannot increase muscle size? Does it mean that with training they cannot build strength? Or maybe it means that older women will never be as muscularly defined or as strong as their younger counterparts? Nope, not according to much of the research. That would be too logical. What these studies seem to mean by difficulty building muscles is that their particular surrogate marker(s) for muscle diminishes naturally across time, in the absence of specific muscle-building activities, and as estradiol, declines(here, here, here, here, here, and here). Well, duh, on so many counts. Of course muscle mass and strength decline across time with disuse or absent activities designed to build muscle and of course estradiol declines with age. We don’t magically build muscle when we are younger just because we are younger, save perhaps when we are children and still growing. That is not how muscle grows in adults. Neither do we magically grow muscle just because we have more estradiol or even testosterone absent training. One has to train the muscle to grow it and train it in specific ways.
As I dug into the literature, it became clear that many of these studies, even when humans were included, which often they are not, never measured anything close to actual muscle development. Currently, the preferred surrogate marker for muscle development is accelerometer readings. Yes, accelerometers. Study participants wear accelerometers that sense change in activity level, and using some entirely-too-complicated metrics, calculate energy expenditure based upon the change from sedentary to active. From there, researchers would estimate what is deemed ‘moderate to vigorous physical activity’ (MVPA). From what I can tell, one can achieve this desired MVPA with about ~40 minutes daily of general exercise including brisk walking, heavy cleaning or gardening, biking, dancing, or other aerobic activity. This is not strength training. It’s just not.
In the past and in less well-funded studies, surveys of physical activity were used. I should note that these two metrics do not correlate. Grip strength is another favorite (here, here), along with various measures of isokinetic strength, using mostly cross-sectional designs. Then there are the slew of studies whose sole purpose appears to convince us that menopausal muscle decline requires hormone replacement (HRT). These too, fall significantly short both in design and their intended purpose of promoting HRT. None of these studies involved any actual strength training, just random assessments of, what I would argue, are random surrogate markers of ‘strength’ (here, here, here, here). In one large study assessing ‘muscle strength’ (N=654 men and women ages 20-93) the researchers noted:
“Only a very small percentage of subjects (<1%) participated in any type of regular resistive exercise, and there was no significant difference in participation by age or gender.”
Less than one percent of study subjects participated in any sort of resistance training and yet the study concludes that both men and women lose strength as they age. Well yes, of course, they do. Disuse across time, no matter the age equals a loss of strength. That does not mean though that age is the variable of concern. Rather, it indicates that if we do not use our muscles, they atrophy.
Of the few studies that I could find with protocols involving strength training in actual older women, we do see muscle growth but it is not as significant as one would expect and perhaps hence, the ‘difficulty building muscle’ conclusion is reinforced. Here again, though, the strength training protocols employed, are not typical of what we would see used to build maximal strength, even when the titles of the studies suggest otherwise. The programs involved using lower weights, machines, and rep schemes that do not accord with strength training programs used in younger or even older lifters. They do not even accord with hypertrophy or bodybuilding programs. It is as if in the very design of the program, the bias that older women are weaker and thus require fundamentally different types of exercises to build strength than younger women or men, determines program design. Admittedly, age plays a role in how one trains, but not in the way that seems to be perceived by the research community.
If we define building muscle as a measure of strength, then we have to design programs to build maximal strength, not just everyday activity strength. If we define building muscle as a bodybuilder might in terms of definition and size, then we have to design the programs to develop muscle in that capacity. If, however, we define muscle building more amorphously, as something to do with overall fitness or functional life capacity, then we are not necessarily ‘building muscle’. We are building overall health with some muscle capacity along the way. This is not necessarily a bad thing, especially compared to a sedentary lifestyle, but it does not answer the question of whether older women can build muscle or strength. It simply does not. And it should go without saying, we must include nutritional protocols as well, particularly protein intake. Training and nutrition cannot be separated if we are building muscle, and unfortunately, nutrition is rarely addressed in these studies.
Can Menopausal Women Build Muscle?
As an older female who lifts heavy and continues to get stronger and more muscular year after year despite my waning hormones, the answer is yes. Menopausal women, when trained appropriately can build muscle – a lot of it.
I came to strength sports late in life, just a few months shy of my 48th birthday, in that perimenopausal period where the rate of muscle loss is purported to increase. As a lifelong swimmer and water polo player, who worked out in these and other sports 6-8 hours a week for most of my life, I was never sedentary for very long. Aerobically, I was in great shape, a little overweight, but I could hold my own in the pool in the fast-paced, high-intensity sport of water polo. By the standard measures used to quantify muscle-building activities in the research cited, I was well above the norm for my age, but was I strong? I thought I was, but when I first stumbled into a CrossFit gym, I found out just how wrong I was. The first time I swung a kettlebell, it was 15lbs and I thought it was heavy. I was genuinely afraid my grip would loosen and I would throw the kettlebell across the room. The first time I deadlifted, 65lbs about killed me. Remember, by the measures cited above, I should have been strong. I wasn’t. My muscles had not been trained for strength.
Fast forward 4 1/2 years or so, I have a little over three years of powerlifting training under my belt and at 52 years of age, I regularly swing 100lb kettlebells and my deadlift currently stands at 342lbs. I also have every intention of pulling 400lbs in a few years. Contrary to the expectations of the academic community who suggest a rapid decline in muscle capacity as we age and as we lose estradiol, I have no difficulty building muscle or strength, despite my declining estradiol concentrations, and though I continue to get older, I am getting stronger. Why? Because I train for maximal strength. It is not as radical as it seems. If one trains to get stronger, strength happens. Of course, I eat right, but mostly, it is because I train and I train hard.
Arguably, an N of 1 is little more than anecdotal evidence. It tells us nothing. I could be unique, an outlier. I am not. I am not even that strong compared to other women in my age group and older. I know 60-year-old women who can rep my max weight like it is nothing. How do I know this? Well, from multiple sources, none of them academic and none of them constitutes evidence as of yet but they are all worth considering as each chips away at the paradigm of inevitable menopausal muscle decline.
The first bit of evidence, master’s powerlifting is a rapidly growing sport for women. A quick glance at an organization that tracks powerlifting records across federations, we see that some phenomenally strong masters’ age women, lifting ridiculously heavy weights. In my age and weight, drug-tested class, the top female lifter deadlifts over 500lbs, and many pull over 400lbs. Remember, these are women in their 50s. Menopausal muscle decline? I don’t think so. Across all weight classes, there are over 3100 female lifters over the age of 50, the oldest listed, is 92 years of age. If this many women are competing, how many others are not? Well, if we look at the CrossFit demographic data, we see that women aged 45 and older make up about 7% of their market. With approximately 4 million CrossFit enthusiasts worldwide, this equates to about 280,000 peri-menopausal women lifting heavy barbells. I suspect many of those women have built significant muscle and strength, certainly more than the women used in academic research or the regular gym-going women whose trainers abide by the menopausal weakness bias and limit their clients to those silly 1-5lb dumbbells.

The second bit of evidence, though again non-traditional, about a year ago, I started a Facebook group and website for older female lifters. We currently have over 5100 women from all over the world. We post our workouts, and our meets, and generally help each other navigate lifting while older and female. The largest segment of the group is women in their fifties, followed closely by women in their sixties.
Among the members of this group, we have women who began their lifting journeys late into their 60s and sometimes even in their 70s. We have many 70-year-olds who can deadlift over 200lbs, some are approaching 300lbs. We even have a 120lb, 80-year-old woman, who began lifting in her 70s and now can deadlift over 200lbs with a fair amount more ease than most 20-year-olds. And oh, most of us squat, bench too. Many of the women in our group compete in the Olympic lifts too and we have others who compete in Strongwoman events. Given the opportunity, older women can and do lift heavy.
Figure 2. Older women who lift heavy.

If any one of these women were tested for muscle density and capacity change across time, we would see legitimate and likely statistically significant changes in both. We would also see that while hormones, nutrition, and other factors co-vary and interact, the most important variable would be the training itself, and the most important aspect of the training is that it is done to increase maximal strength. It is not done for general fitness or weight loss, though those are often happy side-effects, the training we do is to lift as much as possible. Period. Measure that and the myth of menopausal muscle decline goes by the wayside. I would argue that while muscle decline coincides with aging and hormonal decline, it is more attributable to disuse than either of those two factors. The capacity to build muscle exists, even as we age and even after longstanding disuse. It just has to be trained.
Bottom Line: Use It or Lose It
It’s really that simple. Menopausal women can build muscle and strength. We are only limited by whether and how hard we are willing to train. So, if you are an older woman considering lifting weights, do it. Find a coach, put in the time and you’ll be pleasantly surprised just how strong you are. All of us at old ladies lift are here for you. Find us on Facebook @oldladieslift or online at OldLadiesLift.com. If you are a coach or trainer, don’t dismiss the older woman who wanders into your gym and says she wants to lift heavy. She can and she will. Need more proof, take a look at some of these videos. Finally, if you are a researcher who wants to study strength changes in older women, contact me. It’s time to put the myth of menopausal muscle decline to rest.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, and like it, please help support it. Contribute now.













Thank you for this article! Prior to the pandemic I got involved with a gym that encourages women (and men) to lift heavy and also has a bodybuilding competition component to it. There are close to a 1000 women who are in their 40’s 50’s + 60’s and older and younger too, that can attest to what you are saying here! These women safely with the help of trainers get into their best shape and get the strongest they have been in their lives. With good advice re eating adequate protein and all fresh veggies and fruits and healthy fats, I competed in my first bikini competition in 2015 at 47 and then for the next few years (up to the pandemic) I continued to get even stronger. I was crazy strong at 52 then the pandemic hit and then I slipped up my consistency (which is the secret of lifting, just showing up consistently and slowly and carefully upping your weights) I gained a lot of weight (fat) sort of fell off the wagon. I am now climbing my way back to strength at 54 / 55 and am hoping to get back to and surpass where I was when I stopped. Your article is inspiring me! I play tennis, ice hockey bike etc. and lifting heavy makes those activities feel so easy.
On another note. I must say that when I read the research it can have a self-fulfilling prophecy on older women. It almost happened to me!! I catch myself sometimes believing the bs even though I was proof (through menopause also) that I was getting stronger. I had a belief in the back of my mind that my flabby body was the result of being a menopausal woman rather than the truth, I was sitting around eating candy and drinking alcohol more regularly. When I was younger, I did not eat a lot of candy, I was running around playing and being active and I certainly did not consume alcohol. People like to delude themselves 😉 and feel sorry for themselves when they are doing unhealthy activities that are directly responsible for the state of their bodies.
I take hormones, estradiol and progesterone and thyroid. For a while I took testosterone as I didn’t make any. It helped me in so many ways, I went to gym did weights with a trainer, lost 106 lbs in a year, felt great. Fast forward 4 years later, gyms closed from plandemic, doctor refuses to prescribe testosterone anymore since she says It’s normal not to have any at my age (62) well I feel like crap, I gained 30 lbs and I can’t have organs anymore, and I have a 40 yr old husband, this is Not good! My adrenals are “burnt out according to docs, I have adrenal dysregulation and it’s terrible. I lost my muscles and am fat and flabby, I don’t eat sugar I need Testosterone. I ordered Shea I’m hoping it will turn into Testosterone for me. It’s not available in Canada but I’m hoping my order will get shipped. Huge difference in body composition without T. I don’t make hor,ones I have to supplement them.
Find another doctor asap! Lots of online resources too it seems, like Winona. Don’t give up!
I was never overweight as a child or teen, at 20 yrs old I’d put on some weight during pregnancy and by the 2nd child at 22 yrs old, I was exhausted & very out of shape. A few yrs later, a few knee injuries and undiagnosed hypothyroidism and more weight accumulated. Suffice it to say, I spent the rest of my adulthood battling, mostly unsuccessfully, excess weight and poor health. At 49 I went low carb and lost 50 lbs in 4 months, I also started watching bodybuilding videos and joined a gym. Within a year I lost 139 lbs and put on more muscle (ALL naturally) than I ever had in my fittest days as a teen or young adult. I’m 4’11” and at 50 yrs old I was deadlifting
185 lbs, 3 sets of 10 and shaming the 18-25 crowd of fit young men at our gym. No other females, young or older were lifting, certainly not more than a 5 lb weight. I didn’t realize that was considered a lot of weight to lift for someone my size and especially my age and considering I’d only been there 8-9 months at that point. The only time I got on the treadmill was to do a fast, inclined walk for 15 minutes and honestly I got more cardio from the weightlifting. Previous to getting in shape my orthopedic surgeon was only urging me to lose enough weight to do two knee replacements and possibly a back surgery. Eleven years later I still have not done any of those surgeries. I completely changed my body composition, I had muscle that was defined and could be seen, but certainly not bulky or manly looking and I felt strong. I realized that most of the exercise advice touted in women’s magazine’s and by doctors is pure stupidity. I was also warned not to do heavy weight squats and of course didn’t listen, my back got stronger and all the pain that had plagued me for decades was gone. I’m not anti science or anti medicine, but the current medical protocols and advice help nobody. The medical community and standardized medicine is a joke and that’s being nice.