
My husband developed severe vertigo after the second dose of the Pfizer vaccine. Vertigo is a disabling condition marked by a sensation of spinning and disequilibrium that is believed to be caused by inner ear, eye, and/or cervicogenic disruptions. Vertigo has an estimated incidence rate of 64 per 100,000 per year or about 2.4% across a lifetime. The incidence rate of post-vaccine vertigo for the Pfizer vaccine is approximately .8%. Assuming that most of the reactions occur with the second dose, with over 281 million doses (140 million second doses) given in the US when he developed vertigo, we get at least 1.1 million cases of vaccine-induced vertigo. That is 1,100 cases per 100,000 – well above the average incidence rate. In as much as reporting to VAERS, the vaccine adverse events database is voluntary and is said to represent a mere 1-10% of total cases, the numbers could be much higher.
A work colleague of his developed Guillian-Barre Syndrome (GBS) around the same time. GBS is an autoimmune condition attacking peripheral nerve myelination, causing weakness and paralysis. This was also after the Pfizer vaccine. The rate of post-Pfizer/COVID vaccine GBS is ambiguous. One study estimated the rate of GBS after COVID vaccination to be anywhere from 1 case per million to 53 cases per million. Another study calculated the rate to be 20.5 per 100,000 person-years. Person years is a funky calculation that allows estimates of incidence in groups of people across time. Despite the confusing nature of the calculation, what these results tell us, is that with the COVID vaccines the incidence of GBS has escalated and is a least 10-20X higher than it was previously and given the scale of the vaccination program, we’re likely to see exponentially more cases than ever before.
Medication and Vaccine Induced Vertigo and GBS
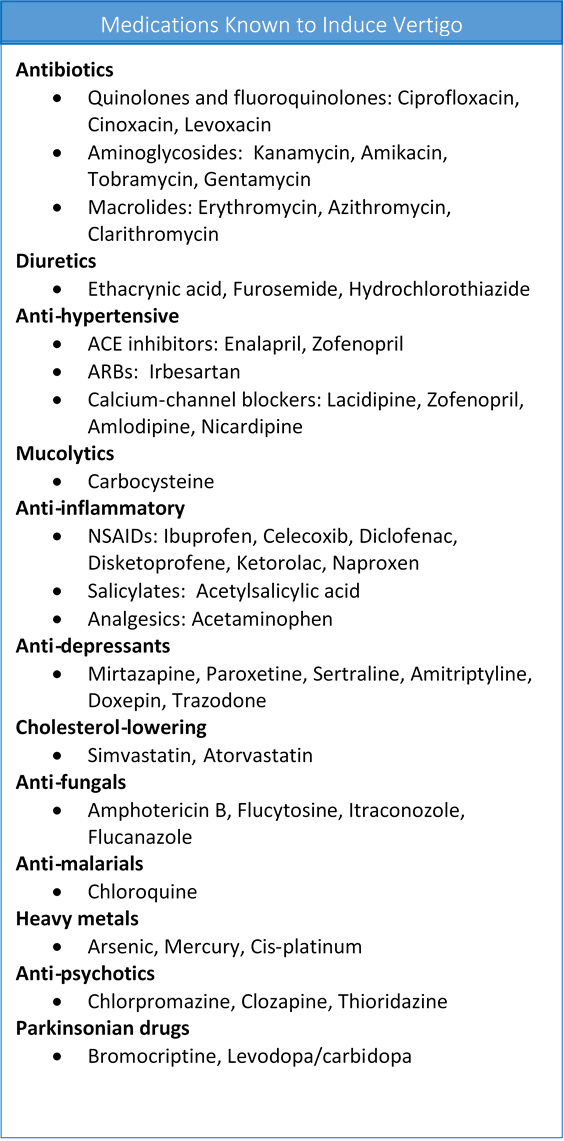
Prior to the COVID vaccines, both conditions had been attributed to an array of precipitating factors including viral infection, vaccines, and medication adverse reactions. The list of medications and vaccines capable of causing either vertigo or GBS is long, so long that it is difficult not to wonder if pharmaceuticals underlie the majority of cases for both of these disease processes. Figure 1. details some of the medications capable of inducing vertigo. A more extensive list can be found here.
A study in 1996 found GBS induced after a variety vaccines including: influenza, tetanus, hepatitis B, rabies, oral polio, measles, mumps, and rubella, and the haemophilus influenzae B conjugate vaccines. Medications that were recognized as causing GBS at the time included: streptokinase, corticosteroids, danazol, captopril, d-penicillamine, oxytocin, and cantharidin. Medscape lists vaccines and fluoroquinolones as possible culprits, but here again, the research is equivocal.
Regardless, neither condition is considered together or as having any common mechanisms. Frankly, until recently, I believed they were separate disease processes altogether. Now, I am not so sure. They may be different manifestations of the same or a similar process: nerve demyelination triggered by mitochondrial depletion in the affected area.
Why do I think they might be similar? When we consider how many fundamentally different formulations of pharmaceutical chemicals initiate one or both of these reactions, it suggests that these reactions are not simply an outgrowth of the chemical’s mechanisms of action. It also suggests that these reactions are not likely to be simply off-target effects that were somehow either missed or undisclosed by the manufacturers. Rather, I suspect these reactions go deeper, to some ‘final’ common pathway that all drugs, vaccines, or really for that matter, severe stressors elicit. It’s not that these drugs are not culpable, they are, just not in the manner we are accustomed to believing.
We are used to viewing drug reactions relative to the drug’s specific mechanisms of action. That is, the drug blocks or upregulates this or that receptor or channel and so we believe that adverse reactions and/or the illnesses initiated develop directly in relation to those actions. Sometimes reactions develop beyond the mechanisms for which the drug was purposed. These are considered ‘off-target’ effects. Off-target effects imply that the drug’s actions affect the functioning of systems beyond what they were designed for. As an example, let’s say a drug was designed to regulate calcium (CA2+) channels in the heart in order to control blood pressure. Off-target reactions would be those that involve Ca2+ channels elsewhere in the body. In reality, since all bodily systems are conserved and thus repeated in all tissue, there is no such thing as an off-target effect. These effects are simply drug effects. Labeling these effects ‘off-target’ is nothing more than a sleight-of-hand meant to distract us from discernment, but I digress.
For vaccine reactions, much of the adverse reaction research focuses on the potential toxicity of the ingredients used to carry/deliver, maximize and/or preserve the viral components. Called adjuvants or excipients, these extra ingredients are often toxic to varying degrees, but they boost immune response (because that’s what happens when the body recognizes toxins) so that is why they are included. As one might expect, these products contain a long list of adjuvants, any one of them is capable of evoking illness under any circumstances, but especially when the individual into whom they are put, has underlying health issues.
The mRNA vaccines are a little different. While they have noticeably fewer ‘ingredients’ than traditional vaccines, they contain a form of synthetic mRNA wrapped in polyethylene glycol nanoparticles that are used to precipitate ‘immunity’. The mRNA tells the body to make COVID spike proteins so that immune cells recognize them and will have the ability to mount an effective attack when presented with the real viral spike proteins. None of this matters, however, with regard to either vertigo or Guillain Barre or any other side effects observed with these products. This is not because they are not without risk, they carry plenty of risks, but because with so many fundamentally different products causing the same reactions, it cannot be the formulation of the product itself per se that is solely responsible for the illness. It has to be an interaction between the host and the product.
Calcium Channel Disruption: A Final Common Pathway?
In previous posts, I explored the role of calcium (Ca2+) channel disruption in the COVID heart and in thiamine deficiency/repletion protocols. In both cases, mitochondrial energy failure causes disruption in the sodium/potassium pumps, which then causes a rapid and uncontrolled influx of Ca2+ into the cells. In case of the cardiomyocyte, this leads to impaired contractility, cell damage, and if not resolved, cell death. I believe a similar process is involved in demyelinating disorders. Here though, instead of occurring in the heart, perhaps because of other genetics or environmental factors, the myelin sheaths of the axons are affected. Some evidence suggest that I am correct.
Mitochondrial dysfunction can leave the axon vulnerable as observed in acute and chronic stages of MS (red). It is hypothesised that the failure of the Na+/K+ ATPase, possibly due to mitochondrial dysfunction, can lead to increased sodium concentrations in the axoplasm. Reversal of the Na+/Ca2+ exchanger can ensue, resulting in toxic calcium levels and downstream processes with consequent axonal degeneration.
In either case, and perhaps across all negative vaccine and medication reactions, mitochondrial capacity broadly, and the regulation of Ca2+ influx more specifically, sits at the nexus. In other words, the capacity withstand a chemical insult, whatever that insult might be, is determined by the mitochondria’s ability to regulate Ca2+ response. If this is true, then by viewing each of these reactions is separate entities, we are missing the forests for the trees.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.











I have to turn to the work and genius of Hans Selye who considered that cellular energy deficiency was the cause of human disease. Beriberi, the outstanding example of energy deficiency is “the great imitator” and is why use of therapeutic thiamine had varying degrees of success in over 240 diseases that have no known connection with thiamine
Numbers mounting. Disastrous statistics by insurance companies of increased deaths ‘unrelated’ to covid. This is across all age groups. Insurance companies see a 40% increase since vaccine rollout. Embalmers seeing new thick vibrios bloodclots. All since the vaccines. Concerning is only the beginning