

In my ongoing research into connections between maternal DES exposure and male sexual development, I recently obtained a copy of the 1953 Physician’s Desk Reference (PDR), a compendium of pharmaceutical products listed together with their manufacturer’s recommended usage.
“Physician’s Desk Reference is published annually by Medical Economics, Inc., through the courtesy of the manufacturers whose major products are described in section 4. It is distributed to over 130,000 active practicing physicians and the pharmacies and libraries of over 4,000 hospitals throughout the United States and its possessions.”
On page 464 is pharmaceutical giant Eli Lilly’s entry for DES, which I’ve scanned and inserted below. Several other manufacturers have their own branded version of DES (for instance, Boyle & Co’s “Hi-Bestrol” DES in 25mg uncoated tablets, for threatened and habitual abortion, supplied in bottles of 100 and 1,000). However, I will concentrate on Lilly’s entry, since they were the major manufacturer and distributor of the drug, and have provided a lot more detailed directions for prescribing the drug than the other manufacturers.
Uses and Dosing for DES According to its Manufacturer
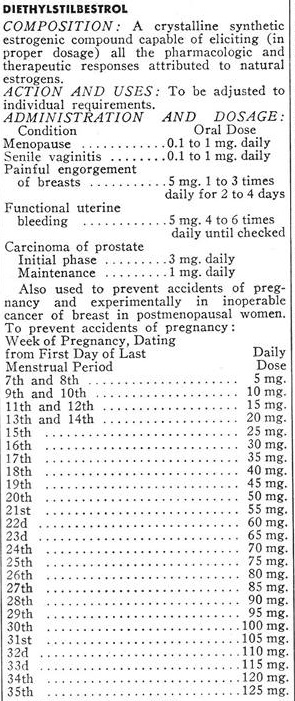
Lilly specifies a variety of uses for DES: Menopause, “senile vaginitis”, painful engorgement of breasts, functional uterine bleeding, carcinoma of the prostate, and to prevent “accidents of pregnancy” (miscarriages). In addition, they helpfully provided a recommended dosing schedule, based on the one devised by Drs. George and Olive Smith were two of the chief proponents of the use of DES to prevent miscarriages. The dosing schedule involves a progressively increasing exposure to the drug, starting at 5mg per day, and progressively increasing as the pregnancy continues until it reaches 125mg per day in week 35 (I guess because, after week 35, the baby is sufficiently well developed that it doesn’t matter if it is born early).
High Dose DES and the Male Fetus
DES is one of the most powerful estrogens ever developed, and even 5mg represents a high dose. You can tell that by the way most of the other recommended uses involve doses considerably smaller. Treating the symptoms of menopause, for example, involves doses of 0.1 to 1 mg per day. Treatment of prostate cancer (through chemical castration) involves a starting dose of 3mg per day, and a maintenance dose (once testosterone suppression has been achieved) of 1mg per day.
Particularly during the later stages of prenatal development, a male fetus whose mother was given DES according to this schedule was being exposed to many times the dose of DES required to cause complete suppression of testosterone production in an adult man. This is very important, because male development, and masculinization of the brain, are driven by the action of testosterone produced in a male fetus’s testicles. Prevent testosterone from being produced, and a genetically male fetus will develop as female instead of male, despite the Y chromosome. This was easily demonstrated by conditions such as Swyer’s syndrome and Complete Androgen Insensitivity Syndrome, in which a failure to produce testosterone or a failure to respond to the hormone, results in a person who is genetically male but physically female.
The conventional causes of intersex all tend to act throughout prenatal development. What I believe has happened with DES is that it has caused a form of intersex, but one that is different from any of the usual causes of intersex because it allowed relatively normal male development to take place during the first trimester, but from the end of the first trimester onward, DES exposure was high enough for testosterone production to become profoundly suppressed.
As you can see from the table, by the end of the first trimester, the dose had already reached 20mg per day and was still climbing. Presumably, the placenta provided some protection from the drug, or an early-stage fetus is more resistant to chemical castration by DES than an adult man because 20mg is already several times the induction dose for chemical castration of prostate cancer patients.
Male Genital Development
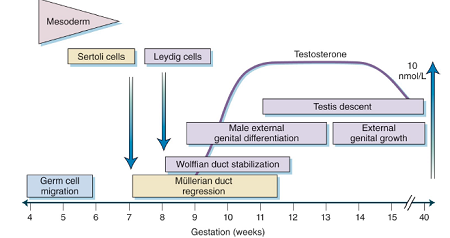
In the figure below, is a chart from an endocrinology textbook showing a timeline of events associated with male physical development. Notice that male external genital differentiation begins in week 7 and has finished by the end of week 12.
During the time genital differentiation is taking place, the main things going on in the brain are very rapid cell division and migration of those cells to their final position in the brain (which is often far distant from where they formed).
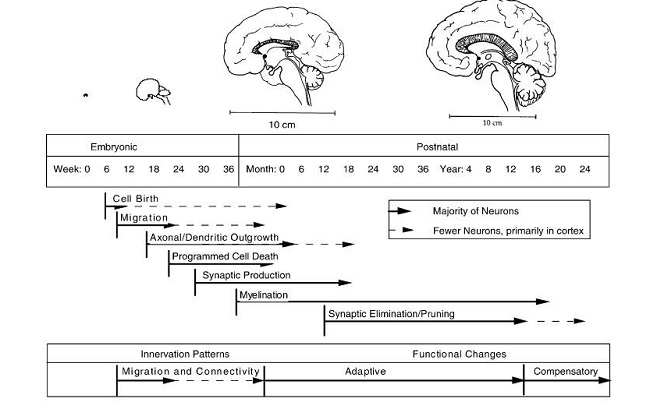
The first elements of the permanent structure of the brain don’t start to be built until about 16 weeks after conception, by which time some brain cells have reached their final position and can start to form permanent connections with other brain cells (“Axonal/Dendritic outgrowth”). I’m guessing that there are two ways of wiring up brain tissue: a male way and a female way, and if there isn’t testosterone present during the time axonal and dendritic growth are taking place, you get the female version.
A process of programmed cell death starts soon after that, which may also be important for whether you end up with a male or female brain. Perhaps certain cells generate aggressiveness and competitiveness, and they only stay alive when excess brain cells are being removed if there is testosterone present. I look at the way men’s faces light up when they’re watching competitive sports, and it’s pretty obvious that they’re experiencing something that I cannot. It makes me think that there could be cells in their brains that generate that “joy of sport”, which were culled from my brain because there wasn’t any testosterone present when their thumbs up or thumbs down moment arrived.
From these two diagrams, it is evident that the first trimester is the key time for genital development, while brain development with regards to gender comes much later and corresponds with the ever-increasing dosages of DES. With these progressively increasing doses, along with the known effects of synthetic hormones on brain development, a good argument can be made that DES may have produced people who are genetically male and look male but have female brains. From talking to people with a known or suspected history of DES exposure, it certainly looks like that is what happens.
DES was used somewhere in the region of 10 million pregnancies worldwide. The schedule published in the PDR wasn’t used in all of them by any means, but it was the manufacturer’s recommendation, and many doctors must surely have followed that recommendation. This raises the prospect that there could well be several million people alive today who look male but have female brains, as a result of the use of DES.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, and like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
This article was published originally on December 12, 2017.












I know this comment is very late in coming but I find your work on DES very interesting. My mother took DES during her pregnancy of my older brother, after having miscarriages between her 1st and 2nd live birth. (the miscarriages were the “indication”) He is about a year and a half older than me. He seemed to be normal, married and having a daughter in his 30s but in his 40s developed an abdominal seminoma the size of a grapefruit (ie testicular cancer tumor in the abdomen, but not in the testis). He had aggressive chemotherapy and recovered. He is now almost 62. I have always thought this seminoma was related to the prenatal exposure to DES. But never found any research on the sons of DES mothers.
My wife is pregnant with a boy, at 14 weeks she started bleeding and the doctor prescribed vaginal Utrogestan 200 mg, once a day. She took it for 2 days before I started reading it might hurt our boys development. Will 2 days have a negative effect?
I think your wife will be fine. Utrogestan is bioidentical progesterone. Although it’s produced in a laboratory, it’s chemically identical to the progesterone that occurs naturally in the human body, and that means it gets processed and metabolised in exactly the same way.
The substances that appear to be causing all the problems with gender bending and other long term health effects, are all synthetic hormones. Synthetic hormones are manmade substances that are designed to stimulate the same hormone receptors that the natural hormones do, but don’t share the same chemical structure (some of them have a fairly similar looking chemical structure, whereas others bear no obvious resemblance to the hormone they’re imitating at all). The synthetics are usually completely untouched by the enzymes, hormone binding globulins and other systems the human body uses to control and limit what the naturally occurring hormones do, and that gives them the ability to cross the placenta and wreak all sorts of havoc on a developing fetus that the natural equivalent wouldn’t necessarily cause.
Another important difference between the natural hormones and synthetics, is that the natural hormones (progesterone in particular) act as raw materials from which other hormones are made, whereas synthetics don’t act as raw materials. It’s a lot like the difference between sugar and saccharin. Both stimulate sweetness receptors and taste sweet, but our bodies can only use one of them as an energy source.
Those two differences probably account for why the synthetics seem to cause all sorts of problems in adults as well as in unborn babies, that aren’t seen with their natural (bioidentical) equivalent. As far as I know, bioidentical progesterone shouldn’t be harmful to an unborn baby (as long as it’s not being given in a dose that would result in an unnaturally high exposure to it). So I don’t think your child will have been harmed.
The work of Ray Peat is also valuable for anyone interested in hormones. I think bio-identical progesterone would be fine too.
Thanks, Hugh, for again pointing out that we are a very nuanced species, and hormones are key to everything.
Accelerated puberty or delayed? Hmm, all those plastic compounds bombarding the human condition (and so many thousands of other compounds and chemicals that supposedly make our lives so much better!) .
We are one retrograde society, for sure, when it comes to sexuality, gender and all points in between. The DES time bomb is yet one of a million possible harms to nature caused by medicine, science, agriculture, and the other polluters.
Here’s a great piece written on a blog I write for regularly, a response to Robert Jensen, UT-Austin journalism faculty who put his foot in his mouth tied to his prejudice and stupidity around what classifies gender and sexuality in an article he wrote, Dexter Thomas:
Here Jensen perpetuates the fallacy that being transgender is a cosmetic issue and motivated by a simple “want” to be female or male, by someone who was not assigned such at birth. However, extensive medical research into transsexuality dating as far back as the 1920s and into present day have demonstrated otherwise, and consequently, medical standards of care have included Gender Reassignment Surgery (GRS) as a necessary procedure for decades. “Gender Dysphoria” is the present name for this condition in the American Psychiatric Association (APA), and treatment follows the standards of care established by the World Professional Association of Transgender Health (WPATH, formerly HBIGDA), which includes GRS. The American Medical Association has also stepped forward advocating the necessity of surgery and its coverage. In fact, like the AMA, the American Psychiatric Association also support GRS as a medically necessary part of treatment.
Treatment of Gender Dysphoria incorporates surgical and endocrine intervention, because analytical and aversion therapies have historically proven damaging. The futility and harmfulness of electroshock therapy, anti-psychotic drugs or conversion (“ex-gay”) therapy is well-documented: modern medicine has realized that this approach simply does not work, and usually results in suppression, suicide or extreme antisocial behavior. Aligning body to mind for this sub-population of the trans* spectrum, however, can work.
Gender Dysphoria is currently (and controversially) listed as a mental health issue, but as I mentioned earlier, ongoing study of both genetic ”brain sex” and Endocrine Disrupting Chemicals (EDCs) show the possibility of some biological causal factors. For instance, a researcher famous for his groundbreaking work in phantom limb syndrome has provided a great deal of evidence that the brain has innate, hard-wired templates for human anatomy. He reasoned that this hard-wired template may also be responsible for a person’s internal sense of gender and how this relates to one’s sexual anatomy, “both of which develop through different biological mechanisms, probably in utero”. Ultimately, he found support for this hypothesis that one’s internal sense of gender and sexual anatomical attributes may also be hard-wired in the brain.
Studies of EDCs show another, possibly concurrent potential that exposure to chemicals that simulate hormone characteristics can affect the signals sent out to determine psychological gender and biological sex, which appear to develop at different times during gestation. In all fairness, nothing is conclusively proven at this point (for the etiology of transexuality OR cissexuality), but a growing body of empirical data from EDC and brain studies tends to support an innate origin or component of intersexuality, transsexuality and cissexuality. I provide this information only to demonstrate the wide spectrum of diversity in nature — not to infer that an understanding of the etiology of homosexuality, heterosexuality, transsexuality, cissexuality, or any other variation is a prerequisite to respecting our basic rights and freedoms.
There is more. Without GRS, many transsexuals experience severe logistic limitations — for example, with employment, where we can go (i.e. the gym, public restrooms, swimming pools), difficulties in establishing relationships, in hospitals, or in prisons that house by physical sex rather than gender identity creating potentially risky or extremely isolating situations. There is also an extremely high risk of violence faced upon the accidental discovery that one’s anatomy does not “match” perceived gender. I could go on and on. But in sum, no other supposedly “cosmetic” issue so completely affects a person’s rights and safety.
https://dissidentvoice.org/2014/06/gender-and-sexual-diversity/
Again, we have genuflected at the alter of profit, tech fixes, and lab coat/PhD syndrome. So much in American medicine early on was a shadow of the Nazi Mengele horror, and unfortunately, much of what happens today in medicine and science is that sick principle, and more, but oh so more sophisticated today and pervasive.
I have personal up close experience with fish and gender switching. In nature, it’s amazing. NATURE!
Quote:
WHEN a school of reef fish loses its single male, the largest female begins acting like a male within a few hours and will produce sperm within 10 days. Some other species repeatedly switch back and forth between the production of eggs and of sperm during a single mating. Among deep sea fish that only rarely encounter potential mates, reproduction is often possible only if one changes sex.
Such opportunistic sex changes in fish, once thought to be a rare oddity, are proving far more common than supposed. Conversions from female to male are now known to occur in species belonging to at least 14 families, while conversions from male to female are known in eight families.
Nevertheless, the process by which fish change sex remains a mystery to scientists. ”No one has ever come up with an answer” as to how they do it, Dr. Klaus D. Kallman of the New York Aquarium, a fish geneticist, said recently.
Nevertheless, according to Dr. N. Robin Liley of the University of British Columbia, the sex of a fish or of a reptile is known to be more susceptible to change than that of a mammal or bird. As examples, the sex of a maturing reptile may be determined by environmental temperature, while a school of trout can be made entirely male simply by adding a certain hormone to the water.
http://www.nytimes.com/1984/12/04/science/sex-change-in-fish-found-common.html
Now back to synthetic estrogen, in rivers:
Canadian researchers who studied fish in Alberta’s Red Deer and Oldman rivers found a peculiar effect of pollution on a native minnow called the longnosed dace. Males they sampled contained elevated levels of a protein marker normally only found in females. Also, “…up to 44 per cent of the male fish had eggs in their testes.” In normal circumstances only females produce eggs. One of the study’s co-authors Lee Jackson said, “… it tells us the fish are exposed to estrogen or something that looks like estrogen to the fish.” Mr. Jackson is the executive director of a research facility which creates new approaches for treating wastewater.
The researchers also analyzed water samples from the river locations where they examined the minnows. They found synthetic estrogens from birth control pills and hormone therapy drugs in the river water. In addition, synthetic and natural hormones were found in the water, which could be from agricultural run-off and cattle ranching. The researchers took samples at 15 locations along 600 kilometers of river. Their study indicated the disruptive chemicals could be present in a span covering the entire 600 kilometers of river water.
http://www.care2.com/greenliving/male-fish-turning-female-due-to-pollution.html
Here, a long article on delayed and accelerated puberty in males and females, homo sapiens. You will not find the reasons/causes why, because, unfortunately, in Capitalism, it’s the water, it’s the food, it’s the soil, it’s the air, it’s the vaccines, it’s the drugs, it’s the socialization, all mixed up in that ugly blender that capitalism depends on — “prove it that cigarettes cause cancer . . . ha, ha, ha . . . .”
http://pediatrics.aappublications.org/content/121/Supplement_3/S218