

I was a pediatrician at Cleveland Clinic from 1962 to 1982 and the clinical research, much of which I have published, was done during those years. I can distinctly remember that a patient with autism was considered to be unusually rare at that time. It was a habit of the pediatric staff to meet regularly with the residents in order to discuss clinical cases, particularly those that were uncommon or rare. I remember a case of autism coming up for one of those conferences because of its rarity. No longer rare, there are many ways in which a child can present symptoms, so the disease is now referred to as autistic spectrum disorder (ASD). This may imply that a lot of different disorders are conceived as being within a spectrum, each with a different cause, or it may simply refer to the wide variation of symptoms.
I looked up the statistics on the Internet and found that ASD today affects one in 68 children (1% of the childhood population). Parents who have a child in the spectrum have a 2% to 18% chance of having a second child affected, implying a genetic risk. I took early retirement from Cleveland Clinic and joined a private practice specializing in nutrient therapy. I became active in the group of physicians who are members of the American College for Advancement in Medicine (ACAM, acam@acam.org). A very big fraction of my patient population during those years was many children with ASD. My clinical experience between 1962 and 1982 had strongly suggested that thiamin(e) deficiency was common in the United States, in spite of the general medical opinion that it never occurred. During those years I had worked with an associate, a doctor who worked in the laboratory. Because of my clinical need, he had researched the literature for ways and means of accurately measuring thiamine deficiency. He had initiated a blood test known as transketolase activity and I need to explain this briefly.
Understanding How Thiamine Works and How to Test for Deficiency
Transketolase is the name of an enzyme whose activity is completely dependent on the presence of thiamine and magnesium, both known as cofactors to the enzyme. There are a series of biochemical reactions in which this enzyme plays an integral part. Known as the hexose monophosphate shunt, this series of reactions occurs in red blood cells. By taking some blood from a patient, the activity of this enzyme can be measured in the laboratory and is reported as transketolase activity (TKA). What we discovered was that the TKA could be quite normal when the symptoms of the patient strongly suggested thiamine deficiency. In order to prove that the patient was deficient, there was a second part to the test. Thiamine pyrophosphate (TPP), the biologically active form of thiamine in the body, had to be added to the reaction container and the transketolase activity measured again. If the TKA accelerated, it showed that the enzyme was lacking the necessary cofactor, in spite of it being in the normal range of activity with the first analysis. It was reported out as a percentage increase of activity as compared with the baseline (thiamine pyrophosphate effect or TPPE).
My friend in the laboratory had done a series of control tests on people that were purportedly healthy. His results compared favorably with reports of the test in the literature and these healthy people could have a TPPE of up to 18%. Anything over 18% for the TPPE guaranteed deficiency of thiamine or magnesium, so both of them would have to be supplemented for the benefit of the patient. Unfortunately, laboratories in prestigious institutions presently only do the TKA and assume that the patient does not have thiamine deficiency if the TKA is in the normal range. From my experience, I am aware that they are missing the majority of patients who have this deficiency. The TKA is not a valid indicator of deficiency by itself. Having given considerable thought to this, I concluded that if the enzyme is equipped with an adequate supply of thiamine there should be no acceleration in its activity after the addition of TPP. The only strictly normal TPPE would be zero (i.e. no TKA acceleration). The percentage acceleration of TKA would reveal a gradual deficiency compatible with no clinical significance until a certain increase in TPPE was recorded as being symptomatic of deficiency. Therefore a TPPE of, say, 15% might be more clinically significant in one individual, whereas 20% might be less significant in another individual. The use of the test requires the clinical experience and adequacy of knowledge of the observer.
Clinical and Laboratory Experience
Without thiamine and magnesium as cofactors, the several enzymes dependent on them begin to become less and less efficient. One of these enzymes is essential to energy synthesis and so thiamine deficiency, because it powers pretty well every cell in the body, can literally cause any disease, since energy is integral to all functions of the body. Depending on the cellular distribution of the deficiency, the clinical expression will vary and there is no typical repetitive clinical expression (phenotype) for thiamine deficiency. However, the brain and heart being the most metabolically active organs are therefore much more susceptible to this deficiency. Thus, brain and heart symptoms are the commonest forms of clinical expression. Thus, it can be assumed that any gross deviation of behavior is evidence of electro-chemically driven changes in brain metabolism related to energy availability.
Case Evidence
Many of the children that I saw with ASD had an increase in their TPPE. Most of them with an accelerated TPPE had a TKA that was in the low normal range. When they were treated with thiamine, many of them responded clinically and their TPPE decreased into the acceptable range, so the evidence was published . The case histories of a mother and her two children were reported . The mother was a recovered alcoholic and alcohol is frequently responsible for causing thiamine deficiency. Some alcoholics react to sugar, particularly if there is a family history of alcoholism that suggests genetic risk. She and both of her children had symptoms that were typical of autistic spectrum disorder, but also they all were recognized to experience the clinical effects of dysautonomia. A description of beriberi clearly indicates that thiamine deficiency disrupts the normal functions of the autonomic nervous system (dysautonomia). All of them had intermittently abnormal transketolase studies indicating abnormal thiamine pyrophosphate homeostasis. Both children had unusual concentrations of arsenic in the urine. All of them had symptomatic improvement with diet restriction and supplementary vitamin therapy, but they quickly relapsed after ingestion of sugar, milk, or wheat. All three individuals became aware that their symptoms were related to their dietary indiscretion, but were quite unable to resist their ingestion of the “foods” that they all knew to be responsible for their relapse. The presence of arsenic in the urine was in keeping with our experience in finding the presence of heavy metals in ASD. My colleagues and I were so impressed with thiamine deficiency as a major cause of ASD that we conducted a pilot study, using a derivative of thiamin known as thiamin tetrahydrofurfuryl disulfide (TTFD). Eight of 10 children showed clinical and biochemical improvement .
The negative relationship of the brain with sugar is mindful of a case that I reported in 2016 and whose story appears on this website. A 14-year-old boy was strongly addicted to sugar and throughout the first eight years of his life his repetitive symptoms had been classified elsewhere as psychosomatic in nature. At the age of eight years it had been discovered that he had the relatively recently described disease known as eosinophilic esophagitis. He also had the classical clinical picture of dysautonomia. It was hypothesized that some form of genetic risk, coupled with thiamine deficiency from out-of-control sugar ingestion, was the responsible combination. The vagus nerve, whose course runs from the brain to the spleen, (and beyond) presides over the control of inflammation. The medical literature has reported food allergy as the cause of eosinophilic esophagitis. The vagus nerve requires acetylcholine as its neurotransmitter, a chemical that is derived from the citric acid cycle (CAC), the cellular “machine” that synthesizes energy. In turn, the nerve is dependent on thiamine that is essential for the entry of glucose into the CAC. Lacking the suppressive function of the vagus on inflammation resulted in a failure to suppress it in the esophagus. Thus, it was conjectured that thiamine deficiency was the primary underlying cause of the esophagitis.
Insufficient Energy and ASD: The Three Circles of Health
Mitochondria are very sensitive to environmental stressors such as toxicants, medication, immune activation, and metabolic disturbances suggesting that mitochondria are involved as a cause of ASD.
Figure 1. Three Circles of Health
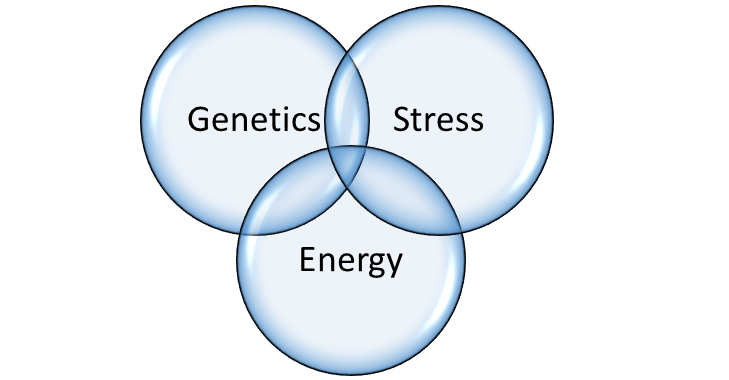
From what has been written above, it must become clear to the reader that I am proposing a very different approach to the cause of ASD and disease in general. It is based on the use of Boolean algebra as represented in Figure 1. This is a statistical method of measuring the influence of variables by representing them as overlapping circles. The individual effect of one circle is represented by its area and its relationship with the other two circles by the area within the overlap. All three circles also overlap, representing the concept that disease might be 100% from one circle alone, by the combination of two defective circles, or by the variable combination of all three.
Genetics
The construction of the human body is based on a code in the form of DNA and represents a “blueprint”. Known as the genome, perfection in the code would create a perfect human body. However, we know that DNA has imperfections, but in most cases a human individual can get along quite well in spite of the imperfections. Although an abnormal gene may be the single cause of disease, the late onset of most genetically determined conditions indicates that an additional factor is required to cause disease expression. This emphasizes the importance of the quality of nutrition in preserving health. For example, type 1 diabetes has a genetic risk, but is not usually expressed for many years, so another factor is necessary. That is why the disease is stress related, making its clinical appearance following something as simple as an infection, a divorce or an injury. Type 2 diabetes often has a genetic risk where either diet or stress, or both, may be initiators.
Epigenetics: Environment and Nutrition
Epigenetics is a relatively new science that seeks to explore how malnutrition and poor lifestyle can have a negative effect on our genes. There are several genetically determined diseases known as inborn errors of metabolism that make their appearance at birth. If any one of them is not recognized in the newborn infant, the result is often a mentally retarded individual. Some of them, perhaps the commonest being phenylketonuria (PKU) require a special diet initiated at birth in order to prevent the mental retardation. That is why in every state in the United States, a special laboratory has been set up to screen a blood test from every newborn infant, in spite of the rarity of the diseases. Sometimes, an infant is born with a gene that creates a risk for generating the disease, but it does not appear unless a secondary factor such as an infection or an injury (stressor) is experienced. There is a disease known as maple syrup urine disease (because the urine smells exactly like maple syrup) that can appear immediately at birth spontaneously or will only appear when the child is hit by some infection or trauma. There are some cases of this disease that respond to megadoses of the vitamin (thiamine/magnesium) that is normally necessary for the mechanism whose failure produces the disease. This has significant importance because a head injury or an infection might be blamed as the sole cause of a clinical problem, whereas the truth could be that the stress factor has initiated a metabolically determined disease previously unsuspected. If such a similar disease responds to the necessary associated vitamin, it can be said that the patient was successfully treated epigenetically.
Stress
In my view, this word is used too carelessly. It is most frequently used to describe the result of stress by saying that someone is “all stressed out”. So let us be clear that stress is some kind of force that a person has to meet and to which an adaptive response is required. It may be a mental force such as a divorce, a business deadline, or a physical assault such as an infection, or an injury. The three circles of health uses the philosophy proposed by Selye. This famous researcher used many forms of physical and mental injury (stress) on rats and studied the biological effects by examining their blood and tissues. He came to the conclusion that each animal went through a process of resistance that he called the General Adaptation Syndrome (GAS). The laboratory results that occurred if the GAS failed to restore health were strikingly similar to those registered in sick people and he proposed the idea that human diseases were the diseases of failure to resist or adapt to stress. What was completely revolutionary was that the GAS required some form of energy to power the machinery that enabled the animal to adapt.
In Selye’s time the biochemical mechanisms of energy synthesis were not well known. Today, these mechanisms are understood and our lives are spent in meeting the daily stresses to which we have to adapt. Our failure to meet the GAS may well be of course that the form of stress is overwhelming, such as a car collision or a virulent infection. However, what we meet on a daily basis is a mental or physical form of stress to which we have to adapt or from which we have to heal. The central factor is the mobilization of sufficient energy to meet the demands of defense. Therefore, the three circles of health predict that the cause of human disease agrees with the concept of the “diseases of adaptation” proposed by Selye.
Energy and the Ability to Adapt
Assuming that the adaptive machinery in the body is genetically adequate, all that is required is sufficient energy to drive it. The symptoms generated during the process of adaptation simply represent the locality of the energy deficiency and constitute a warning by their perception in the brain. They have to be interpreted for their underlying meaning rather than accepting them as the effects of a named disease such as Alzheimer’s or Parkinson’s. Since the brain is an electrochemical “machine”, the nature of the patient’s diet, as well as family history, are essential to beginning to unravel the problem. In the case of ASD, the mother’s diet during pregnancy is of vital importance. Occasionally, a seemingly irrelevant observation by a physician can be valid. I was riding in a car with a gentleman who had a group of infant’s shoes dangling behind the windscreen. I asked: ‘what was the significance?’ He responded by telling me that his first child died in infancy from a rare genetically determined disease. Subsequent children had survived and this was his method of keeping them in memory.
Nutrition as Medicine
When Homo sapiens arrived on the face of the earth, or even when his ancestors were present, the food was available and the general concept is that we were hunter gatherers. To find out what kind of food an animal should be taking, you have to look at the teeth. We have cutting teeth, canine teeth and grinding teeth, indicating that we are omnivores and can consume meat, vegetables and fruit. The necessary non-caloric nutrients (vitamins and essential minerals) were in the natural food. In the modern world, our food is far from natural and the high calorie content, particularly in the form of sweets, is overwhelming the cellular machinery that synthesizes energy. For this reason, many of the illnesses that haunt a physician’s office are merely a reflection of a mild to moderate energy deficiency in brain cells. If recognized for what they represent and treated with appropriate nutrition, the symptoms quickly disappear. If not, we can hypothesize that there may be permanent damage that is diagnosed as one of the neurodegenerative diseases.
The trouble with understanding this concept is that the distribution of the energy reducing mechanism, together with genetic risk, will vary from individual to individual. A child with a genetic risk, or, more commonly, a victim of poor maternal diet, is born a candidate for energy deficiency. That is why ASD can be the result of thiamine deficiency or any other mechanism that interrupts the flow of energy. However, the same deficiency can give rise to many other conditions presenting with an unpredictable array of symptoms. There is a great deal of evidence that food is burned (oxidized) in the cells of the body to create a form of chemical energy (ATP) that is transduced to electromagnetic energy. It is this energy that is used to drive physical and mental action. There is also evidence that a biological form of thiamine (thiamine triphosphate) is important in the electomagnetic transduction process, thus making thiamine uniquely indispensable. It is for this reason that I have spent many years emphasizing the life-giving properties of this extraordinary vitamin. I am not therefore surprised when I read that a constellation of symptoms called Parkinson’s disease has been reported to respond to treatment with thiamine.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.













Does anyone know how on earth you can get a child to take Allithiamine who cannot swallow capsules. The powder is just vile and cannot be hidden in any foods, especially not with a child who has ASD.
I brought the Allithiamine cream to try instead but it is equally problematic, having to keep it outside in garage inside two sealed bags and the whole garage still stinks of the stuff. Cannot use it on weekdays when they are at school and can only use at weekends if they are not going out but then the whole house smells repulsive.
Try thiamine HCl mixed in water.
Cocarboxylase is the form of B-1 that seems to help me the best, followed by Benfotiamine.
Hey Derrick, I’ve heard you talk about the paradox reaction before. I took magnesium taurate with lipothiamin, but I switched to magnesium Threonate which has the ability to cross the blood brain barrier, just like lipothiamin. When I switched to this all my previous symptoms, nausea, back pain, dizzyness and insomnia came back worse. But one thing was extremely weird. My hypersensitivity yo mosquito bites has subsided substantially, almost gone, on the day of supplementation. I took a break from it for a week and came back, not as brash of a change this time but still spikes my symptoms quite a bit.
Paradox is published under the heading of “refeeding syndrome”.The symptoms immediately become worse for an unpredictable period as long as a month. The only remedy that I know is to persist with whatever agent is causing it until the symptoms abate. The exact mechanism is unknown but it is hypothesized that the patient is suddenly changed from a catabolic (nitrogen loss) to an anabolic (nitrogen gain) state, signalling the brain that then reiterates, or exacerbates the symptoms
Cocarboxylase is the active form of thiamin and is made in the body; Theoretically you could have a deficiency if it is not synthesized in the body.
Have you ever seen or can you fathom of a thiamine cocarboxylase deficiency?