

Principles of Energy Production and Consumption
Before we begin the discussion of creatine and creatinine, I would like to begin this post by providing a simple analogy to understand the necessity evaluating a patient’s mitochondrial energy status using the principles surrounding our perception of the family car. You get into the car, start the engine and off you go. This is absolutely expected and will institute anger or irritation if this does not happen. Most people, including myself, are not the least interested in knowing how the car works in its mechanical details. However, we all know that you have to put a flammable liquid in a tank and you have to have a battery. My personal interest is understanding the principles. The engine burns gasoline and produces energy. The battery produces an electric spark that ignites the gasoline. But we also know that the type of gasoline is calibrated to the design of the engine. We are warned not to deviate to another type of fuel because it might ultimately damage the engine. That energy must be transmitted to the wheels by means of a series of levers or metal gadgets known as the transmission. The metal gadgets (cog wheels or levers) require lubrication with oil. With the exception of self-drive, the car needs a driver. Waste products are eliminated through an exhaust pipe. If the car has something wrong that prevents its use, we call a mechanic and the car may be removed to a place where repair can be initiated. Note that the mechanic has to know the practical details of the machinery that enables the car to function.
The human body has exactly the same needs in principle. Differences are in the details the fuel that we need is the equivalent of gasoline and was invented by Mother Nature. The engines of the cell are called mitochondria where the energy is produced. The primary fuel of the brain that guides the body is glucose and this has to be ignited (burned, oxidized). Vitamin B1 (thiamine) is the equivalent of a spark plug. In the analogy, the brain is the equivalent of the car driver and the car represents the human body. The driver controls the car by means of gear levers, accelerator etc.
The energy produced in mitochondria has to be transmitted in order to produce function. The equivalent of a transmission is a biochemical pathway that consists of a series of enzymes (cog wheels), each of which require energy to become active. The elimination of waste products is through the kidney, the breath, the sweat, and the colon. The enzymes that make up energy production and energy consumption all require chemical substances called cofactors and these also occur in the diet as vitamins and minerals. Although a poor analogy, the cofactors might be thought of as like the oil necessary in the transmission of a car. Physical and mental function can be maintained for long periods because energy is being produced and consumed in a state of balance. Disease production is because either energy production or its consumption is failing. The major symptom of energy failure is a sense of fatigue. The equivalent of a mechanic is the physician. Surely, like a mechanic, he needs to know all the details of how the electrochemical machinery produces function and have a working knowledge of how the fuel affects it.
Creatine and Creatinine Ratio as a Measure of Energy Metabolism
There have been many posts on this website that have discussed energy deficiency as perhaps the most important consideration in our attempts to define health and disease. We need to be able to detect evidence for this in a relatively simple way that can be done cheaply in any clinical laboratory. Between 1962 and 1982 I was fortunate enough to be able to perform clinical research and I found a simple method that I will try to explain here. I would hope that an interested physician, indulging in casual reading, might one day come across this post. People suffering from the many disease conditions that have been discussed as energy deficiency might be able to pass the idea on to their personal physician
You can go online and type in “creatine”. You will find an enormous amount of information about this substance. Many commercial preparations are presented and advertised as an agent that can improve fitness, increase energy, or for bodybuilding. The reader looking for the truth may very easily be skeptical and probably rightly so. I will begin by explaining how this substance is made in the body and how it is used. It is mainly created in the liver and kidney and travels in the blood, mainly to the muscles. An energy dependent molecule called a transporter enables it to be absorbed into the muscle where an enzyme converts it to phosphocreatine. Notice that its entry to the muscle is energy dependent.
Now we come to its use in energy metabolism. As most people know, ATP is known as the energy currency because it is this substance that provides the energy to almost all of our cells. When and if there is a phenomenon going on in the body that causes reduced production of ATP, call it “an energy crunch”, phosphocreatine can be used in the muscle to make ATP. Hans Selye would have called this energy crunch a “disease of adaptation”, a war between an attacking agent and the energy requiring body defenses. One might suggest that phosphocreatine is held in reserve as a backup. If it is not required, it slowly leaks out of the muscle in the form of creatinine, which then travels in the blood to the kidney where it is excreted in the urine as a waste substance. The normal state would be a small amount of creatine and a relatively high concentration of creatinine in urine, reflecting that the patient has enough ATP and is healthy. A low urinary creatine/creatinine ratio predicts health, a high ratio predicts an energy crunch or a disease of adaptation.
Normal and Abnormal Energy Synthesis: Understanding the Creatine Creatinine Ratio
If all the nutritional components are present and assuming a healthy genome, glucose is oxidized (burned) and complex machinery produces ATP. If this is an adequate presence, creatine is not necessary. Notice, however, that the mechanism that enables creatine to get into the muscle cell is an energy dependent transporter. So if that mechanism is deficient in ATP, the creatine cannot get into the muscle. It will continue to travel in the blood, eventually reaching the kidney where it will be lost in the urine, just like creatinine. There is always a small amount of creatine in the urine, but if the energy deficiency is affecting its transport into the muscle cell it will be found in an increased concentration in the urine. Herein lies the potential fallacy for creatine as an energy producing dietary supplement. By measuring creatine and creatinine in the urine, a high ratio is a reflection of energy deficiency. Of course, we now have to consider the cause of the energy deficiency, so the ratio does not reveal the cause. It merely states that energy deficiency is the underlying cause of the clinical expression of disease. If a therapy shows clinical improvement in the patient, the creatine/creatinine ratio can be repeated and it will decrease into the normal range as the test is repeated, thus proving that energy metabolism has improved in the patient. Of course, if the patient’s illness includes destructive damage to the kidney, this method of depicting energy deficiency would fail. Theoretically, it would be possible to show a high creatine/creatinine in the blood.
Increased Urinary Creatine in Energy Deficiency Diseases: The Thiamine Connection
Increased urinary concentrations of creatine have been noted in beriberi, thus exposing the fact that thiamine deficiency presents as an energy deficient disease, which has been liberally discussed on this website. In an experiment in rats, creatinuria occurred in protein calorie starvation, but occurred earlier and in much greater amounts if there was associated thiamine deficiency. It is also interesting that creatinuria disappeared in beriberi patients with bed rest, before thiamine had been discovered, thus underlining physical (and hopefully mental) rest for sick people. In children, creatinuria is regarded as physiologic because they have a faster metabolism but it is still valuable in calibrating the rate of that metabolism in the normal versus the abnormal state. Its association with starvation is an obvious reflection of the simple fact that ATP is the product of a healthy genome, good nutrition and that thiamine is a critical nutrient.
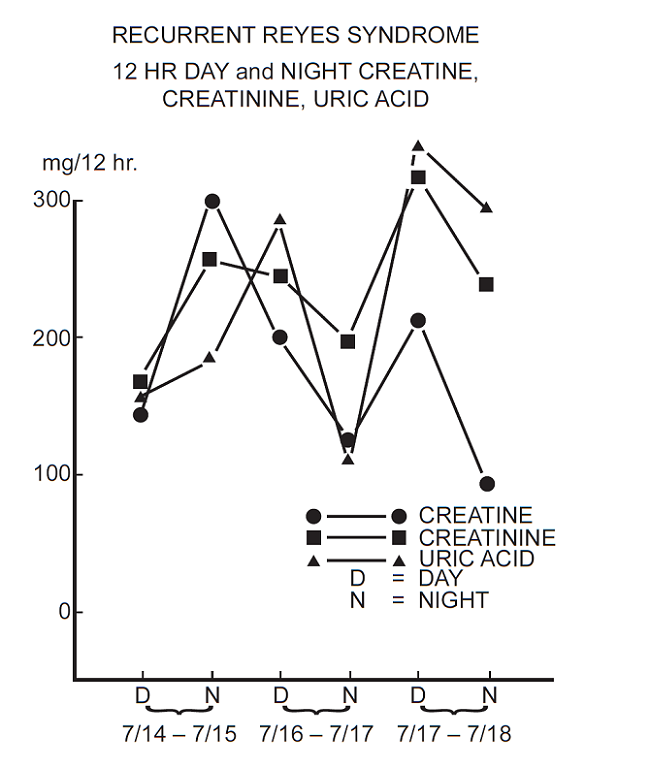
Creatine and Creatinine in a Recurrent Reyes-like Syndrome
Many people reading this post will remember a disease that kept cropping up in association with a virus epidemic such as flu. For a long time it was believed that it was a direct result of the virus but it was later found that it was caused by the aspirin that was being used by parents to bring the temperature down in their child with the viral disease. This comment is probably pertinent in seeing the complications observed in Covid-19 patients. The resultant syndrome is described as an extremely rare but severe and often fatal disease. Death occurred in about 30 to 40% of cases resulting from dysfunction of brainstem. This part of the brain enables us to adapt to the environment and is highly sensitive to energy deficiency. The biochemical explanation for the syndrome is a generalized disturbance in mitochondrial metabolism, eventually resulting in metabolic failure in the brain, liver and other tissues. Thus several infections and diseases might present clinically with a Reye’s-like syndrome. A study using energy-compromised yeast cells found that aspirin starves the mitochondria of an important metabolite in the synthesis of energy. Note the use of the phrase “energy compromised” suggesting the probability that the children that succumbed to Reye’s syndrome were already energy compromised before the viral infection.
Many years ago I was confronted with a 10-year-old boy whose case is described in detail on page 189 of our book. This child had experienced 30 episodes of a condition that was remarkably like the clinical expression of Reye’s syndrome but with repeated spontaneous recovery. A brother had died from a similar condition and another sibling had experienced rheumatoid arthritis that had remitted spontaneously. I studied two separate episodes. The first one was allowed to proceed and recover spontaneously without any treatment. He was discharged from hospital, only to return later with another identical episode. I treated this one with thiamine tetrahydrofurfuryl disulfide (TTFD). In both cases the urinary creatine gradually decreased to normal levels but was much more efficient in the TTFD example.
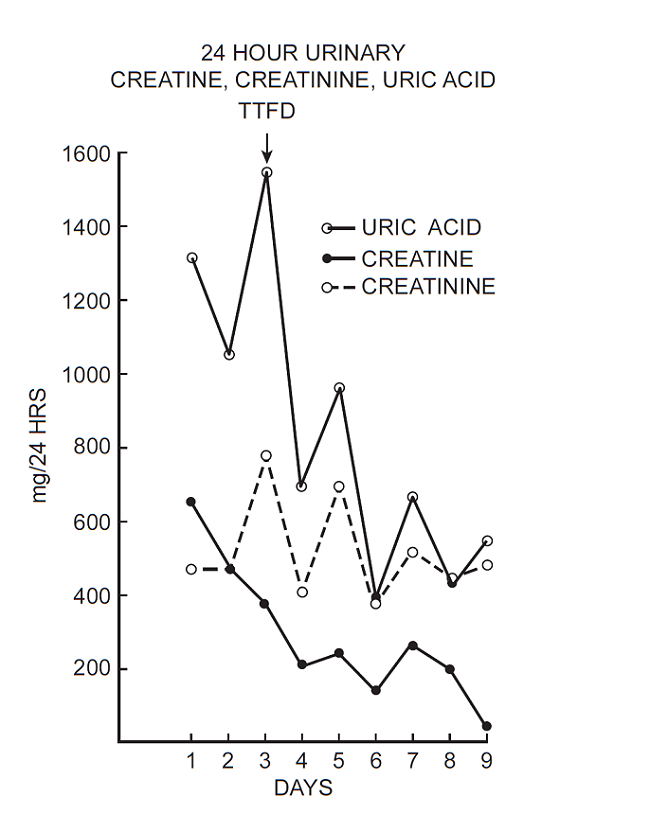
I recommended to the parents that he should continue taking TTFD on a preventive basis but for some reason unknown to me this was discontinued and he subsequently died from one of these episodes. Although I never was able to discover the exact mechanism it was very clear that this was an energy dependent recurrent episode. The repeated spontaneous recovery suggested that, like a patient with beriberi, the creatinuria would decrease into the normal range with rest, because in each case he would be confined to bed.
Improve Energy Efficiency. Improve Health.
The efficiency of the recuperation was improved by the use of the TTFD, suggesting that he was mildly energy compromised on either a genetically determined or nutritional basis, even when he was well. His recurrent episodes suggested an environmental stress factor that compromised his energy output even more and this might of course have been related to diet. How is it that I can draw such a far out conclusion, you might ask?
TTFD is a disulfide derivative of thiamine, a vitamin. Its advantage over thiamine is only in its delivery of the vitamin to cells, but thiamine still has only one overall action in the body. I say overall because its presence has been found in every aspect of very complex cellular machinery that produces energy. Dietary thiamine has to go through many vitally important changes in the body. A phosphate molecule is added to create thiamine monophosphate (TMP) and we still do not know what its biologic function is or even whether it is merely an intermediate on its way to becoming thiamine diphosphate (TDP), which is also known as thiamine pyrophosphate (TPP). This is the only thiamine molecule, as a cofactor for many enzymes, whose action is known and understood. Then it has to have a 3rd phosphate molecule added to make thiamine triphosphate (TTP). I know a scientist in Belgium at the University of Liege whose entire career has been spent on trying to discover the actions of TTP and he is not there yet! One of his group’s discoveries is that it has some effect in electrogenesis (conversion of chemical to electrical energy). Not many physicians are familiar with this important aspect of what makes animals, including human beings, tick and it is extraordinary that so little effort has been made in disease analysis toward the production of energy and its consumption. When I learned that thiamine propyl disulfide (an earlier derivative with the same action as TTFD) had been found to give partial protection to mice from the lethal action of cyanide, I couldn’t help but accelerate my interest in its therapeutic potential.
This kind of thinking leads to a bizarre conclusion. Perfect health is a combination of genetically determined perfection in structure, with perfect energy production. Its imperfection in either or both that fails to meet life stresses that leads to illness. Therapy can only be derived from perfecting the fuel intake and/or stimulating energy production and its efficient consumption. Note that a sibling had rheumatoid arthritis that reportedly remitted spontaneously. It is most unlikely that this child carried genes that were responsible for two different diseases. Also, on page 248 of our book, we reported the case of a girl whose clinical diagnosis was rheumatoid arthritis who responded to treatment with TTFD. Although it sounds like a state of therapeutic imagination, I believe that it strongly supports the fact that our present disease model is either catastrophically outdated or was a wrong interpretation of disease in its origins.
We Need Your Help
More people than ever are reading Hormones Matter, a testament to the need for independent voices in health and medicine. We are not funded and accept limited advertising. Unlike many health sites, we don’t force you to purchase a subscription. We believe health information should be open to all. If you read Hormones Matter, like it, please help support it. Contribute now.
Yes, I would like to support Hormones Matter.
NATASHA HARTANO/FLICKR (CC BY-NC 2.0); ADAPTED BY L. STEENBLIK HWANG











In reference to higher or lower ratios of creatine/creatinine, is there an optimal range?
I came across this question by rereading the post in October. I hope that Katz may come across my answer. When I was in practice I saw quite a few cases of CFS and Fibromyalgia. They usually responded to high dose thiamine and their urine creatine/creatinine ratios were high at outset of treatment and dropped to the normal ratio for the age of the patient after treatment.
September 2022 – read your reply Dr. Lonsdale. Thank you!
Creatine is made in the body and travels in the blood. It is picked up chiefly by muscle and brain where it is stored as phosphocreatine. If there is an ATP shortage, phosphocreatine donates its phosphorus to adenosine anaerobically to make ATP. The creatine travels to the kidney and is excreted in urine in high concentration. If phosphocreatine is not used, it leaks into blood nonenzymatically as creatinine and is lost in urine. Thus a shortage of ATP will cause a high creatine/creatinine ratio in urine as am indicator of ATP deficiency. Using creatine as a supplement will be an inefficient way of restoring energy. The more efficient way of restoring energy would be the administration of thiamine to stimulate aerobic metabolism. A high creatine/creatinine ratio would be a good test for energy deficiency in any disease such a CFS and a fall in the ratio would indicate clinical improvement.
From a 2015 study on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome [ME/CFS]
*”Metabolic profiling reveals anomalous energy metabolism and oxidative stress pathways in chronic fatigue syndrome patients”*:
https://www.researchgate.net/publication/277979239_Metabolic_profiling_reveals_anomalous_energy_metabolism_and_oxidative_stress_pathways_in_chronic_fatigue_syndrome_patients
– “Dysfunctional energy metabolism appears to have impacted creatinine and its elevation in urine suggests that it may be used as an alternative for anaerobic ATP production within muscle.”
– “Creatinine has been used to standardize urinary metabolite concentrations to account for variations in urinary accumulation and dilution factors. In this instance we deemed it an inappropriate method as creatinine was trending towards a significant decrease within the absolute concentration blood data of ME/CFS patients. In this study when the urinary data was normalized to urinary creatinine all metabolites were significantly altered, which we concluded was an artificial result. To remove the influence of dilution factor on both the urine and the blood we normalized each sample to the total metabolite concentration, therefore producing relative abundance data. This method of normalization focuses analysis on the ratio of metabolites within either the blood or urine.”
Dr. Lonsdale – have you had the chance of having an exchange with any of the researchers working on ME/CFS? I get the impression the folk over at Open Medicine Foundation are keen on learning and listening.
So interesting and appreciated. Thank you Dr Lonsdale. ?